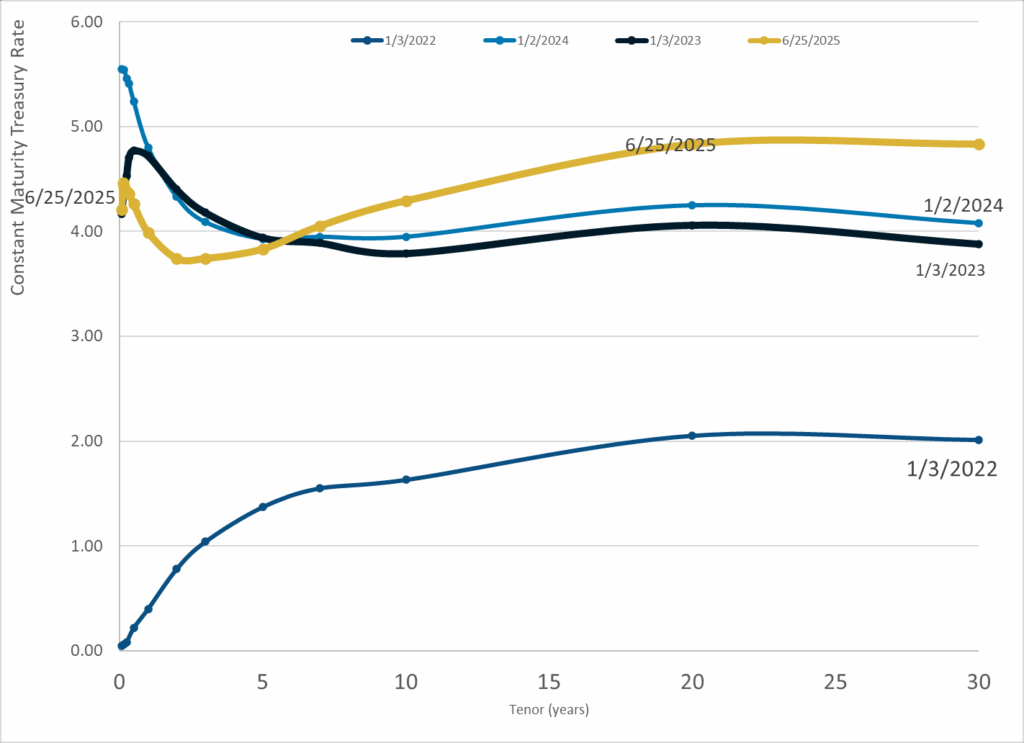
Graphic:

Publication Date: 27 Jun 2025
Publication Site: Treasury Dept
All about risk
Graphic:
Publication Date: 27 Jun 2025
Publication Site: Treasury Dept
Graphic:
Publication Date: 25 Jun 2025
Publication Site: Treasury Dept
Graphic:
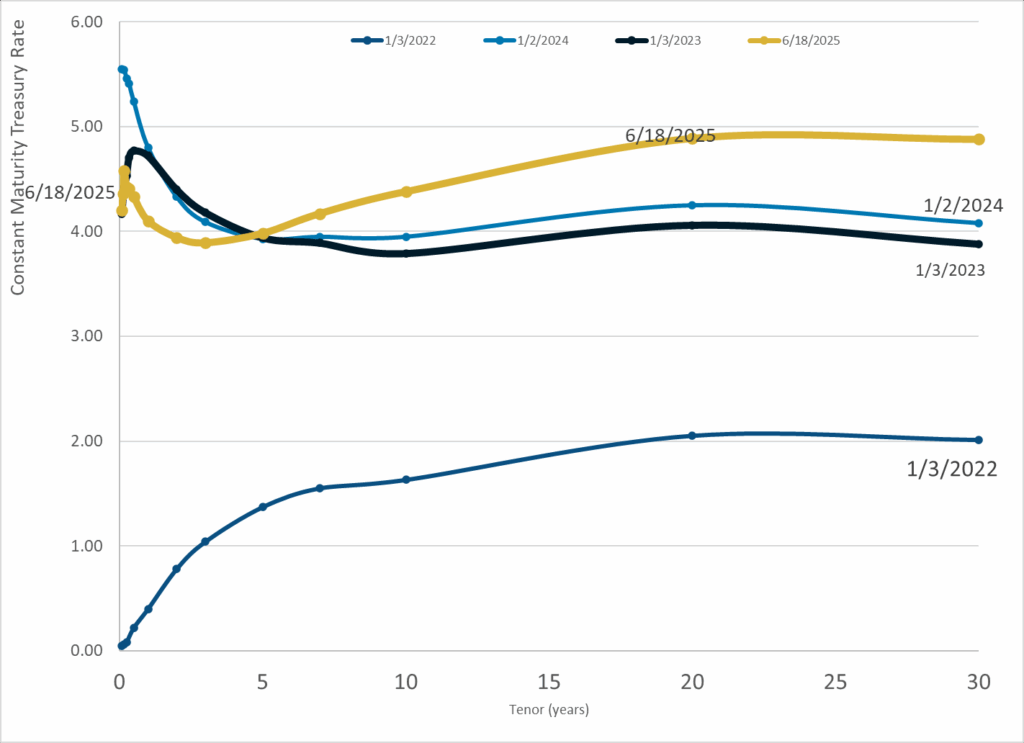
Publication Date: 18 Jun 2025
Publication Site: Treasury Dept
Link: https://www.theatlantic.com/health/archive/2024/07/millennials-cancer-death/678896/
Excerpt:
Several years ago, in my work as a palliative-care doctor, I cared for a man in his 60s who had been mostly healthy before he was diagnosed with stomach cancer. After three different treatments had failed him, his oncologist and I told him that a fourth treatment might buy him a few weeks at best. “Send me back to Boston,” he said immediately. He wanted to smell the Atlantic, see his childhood home. He made it there, dying a week later.
My patient died on his own terms: He was comfortable, fully informed about his worsening cancer, and able to decide where he wanted to die, whom he wanted to be with. This is the type of proverbial “good death” that our medical system is slowly learning to strive for—but not necessarily for younger people.
In the hospital room next to this man was a young mother who, like me, was in her 30s. We bonded over our love of ’90s music and the Southern California beaches where we’d built sandcastles as children and stayed out late as teenagers. She, too, was dying of Stage 4 stomach cancer; I first met her when her oncology team asked if I could help manage her pain and nausea. She would rest her hands on her protruding belly, swollen with fluid and gas because cancer blocked her bowels; she couldn’t eat, so medications and liquid nutrition dripped through a large catheter threaded up a blood vessel in her arm and into her heart.
Author(s): Sunita Puri
Publication Date: 5 July 2024
Publication Site: The Atlantic
Graphic:
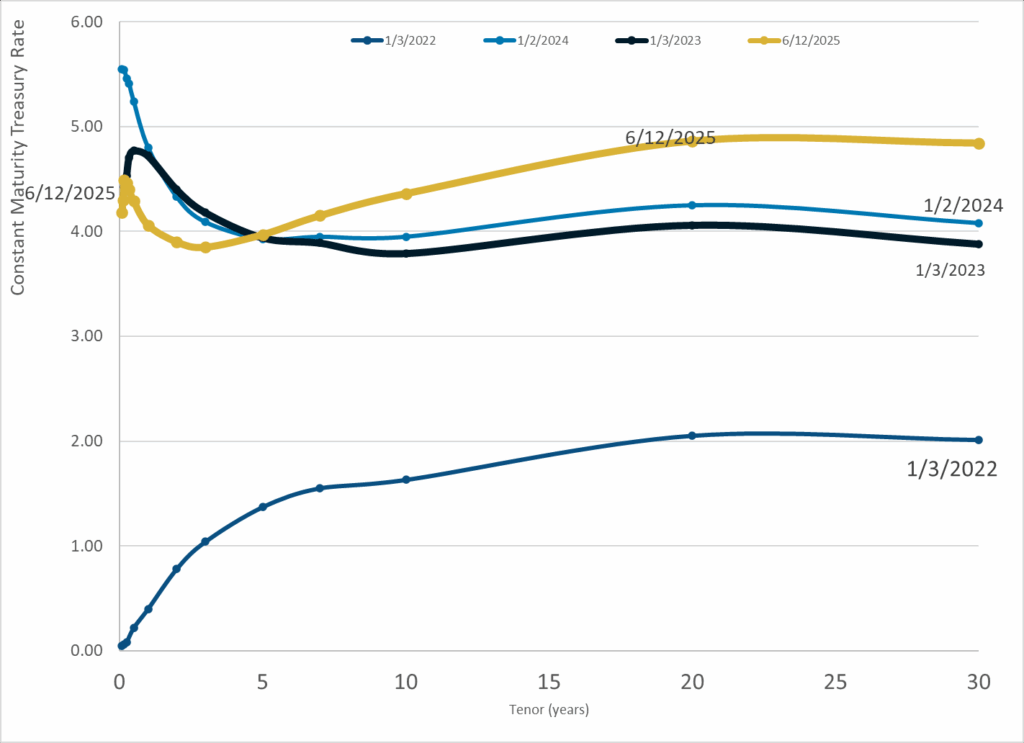
Publication Date: 12 Jun 2025
Publication Site: Treasury Dept
Link: https://www.nber.org/papers/w33905
Graphic:
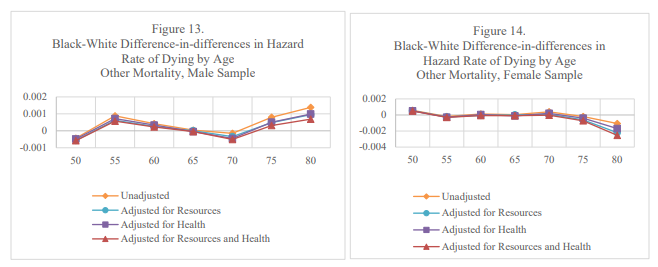
Abstract:
Racial differences in mortality are large, persistent and likely caused, at least in part, by racism. While the causal pathways linking racism to mortality are conceptually well defined, empirical evidence to support causal claims related to its effect on health is incomplete. In this study, we provide a unique set of facts about racial disparities in mortality that all theories of racism and health need to confront to be convincing. We measure racial disparities in mortality between ages 40 and 80 for both males and females and for several causes of death and, measure how those disparities change with age. Estimates indicate that racial disparities in mortality grow with age but at a decreasing rate. Estimates also indicate that the source of racial disparities in mortality changes with age, sex and cause of death. For men in their fifties, racial disparities in mortality are primarily caused by disparities in deaths due to external causes. For both sexes, it is racial disparities in death from healthcare amenable causes that are the main cause of racial disparities in mortality between ages 55 and 75. Notably, racial disparities in cancer and other causes of death are relatively small even though these causes of death account for over half of all deaths. Adjusting for economic resources and health largely eliminate racial disparities in mortality at all ages and the mediating effect of these factors grows with age. The pattern of results suggests that, to the extent that racism influences health, it is primarily through racism’s effect on investments to treat healthcare amenable diseases that cause racial disparities in mortality.
Author(s): Robert Kaestner, Anuj Gangopadhyaya & Cuiping Schiman
Publication Date: June 2025
Publication Site: NBER Working Papers