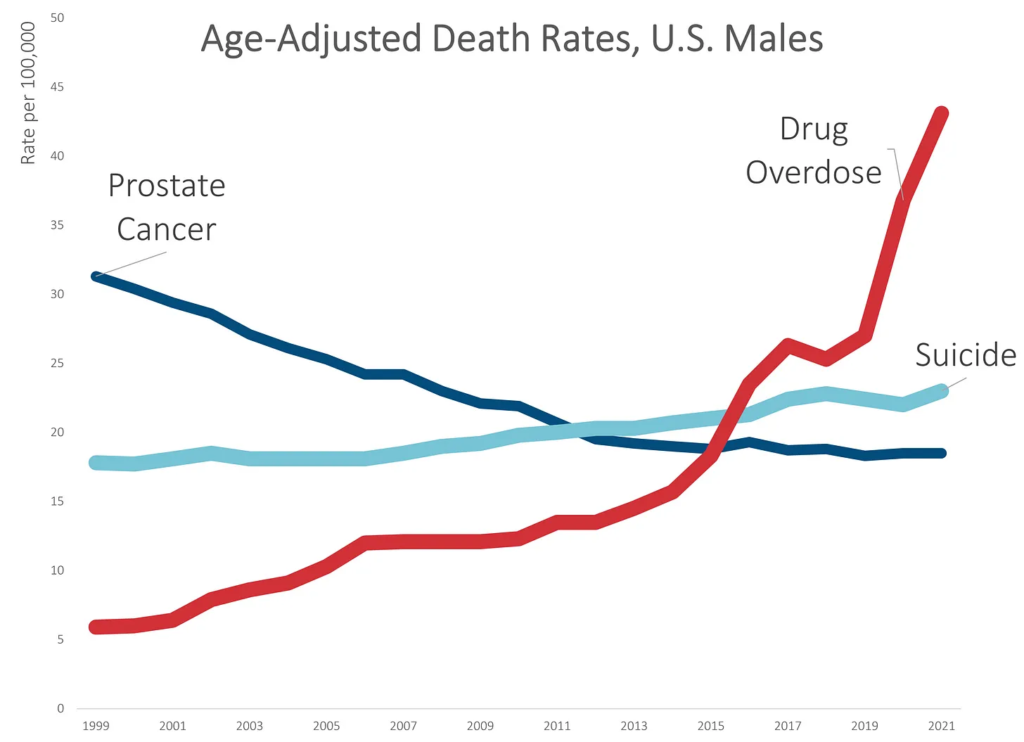
While death rates due to suicide increased by about 30% over the 20-year period, death rates due to unintentional drug overdoses increased by over 500%.
None of this is really a surprise. I’ve written about the drug OD problem many times before, which had a horrible trend before the pandemic and got much, much worse during the pandemic.
Much of the increase came in 2020 and 2021 — over 30% in 2020, and 17% in 2021. These are huge increases on rates that were already bad.
Question Is the incidence of organ donation and transplants higher during major US motorcycle rallies?
Findings In this cross-sectional study of 10 798 organ donors and 35 329 recipients of these organs from a national transplant registry from 2005 to 2021, there were 21% more organ donors and 26% more transplant recipients per day during motorcycle rallies in regions near those rallies compared with the 4 weeks before and after the rallies.
Meaning While safety measures to minimize morbidity and mortality during motorcycle rallies should be prioritized, this study showed the downstream association of these events with organ donation and transplants.
Author(s): David C. Cron, MD, MS1,2; Christopher M. Worsham, MD3,4,5; Joel T. Adler, MD, MPH2,6; et al
Publication Date: 28 Nov 2022
Publication Site: JAMA Internal Medicine
JAMA Intern Med. Published online November 28, 2022. doi:10.1001/jamainternmed.2022.5431
Experts have warned that Europe faces a “cancer epidemic” unless urgent action is taken to boost treatment and research, after an estimated 1m diagnoses were missed during the pandemic.
The impact of Covid-19 and the focus on it has exposed “weaknesses” in cancer health systems and in the cancer research landscape across the continent, which, if not addressed as a matter of urgency, will set back cancer outcomes by almost a decade, leading healthcare and scientific experts say.
A report, European Groundshot – Addressing Europe’s Cancer Research Challenges: a Lancet OncologyCommission, brought together a wide range of patient, scientific, and healthcare experts with detailed knowledge of cancer across Europe.
One unintended consequence of the pandemic was the adverse effects that the rapid repurposing of health services and national lockdowns, and their continuing legacy, have had on cancer services, on cancer research, and on patients with cancer, the experts said.
“To emphasise the scale of this problem, we estimate that about 1m cancer diagnoses might have been missed across Europe during the Covid-19 pandemic,” they wrote in The Lancet Oncology. “There is emerging evidence that a higher proportion of patients are diagnosed with later cancer stages compared with pre-pandemic rates as a result of substantial delays in cancer diagnosis and treatment. This cancer stage shift will continue to stress European cancer systems for years to come.
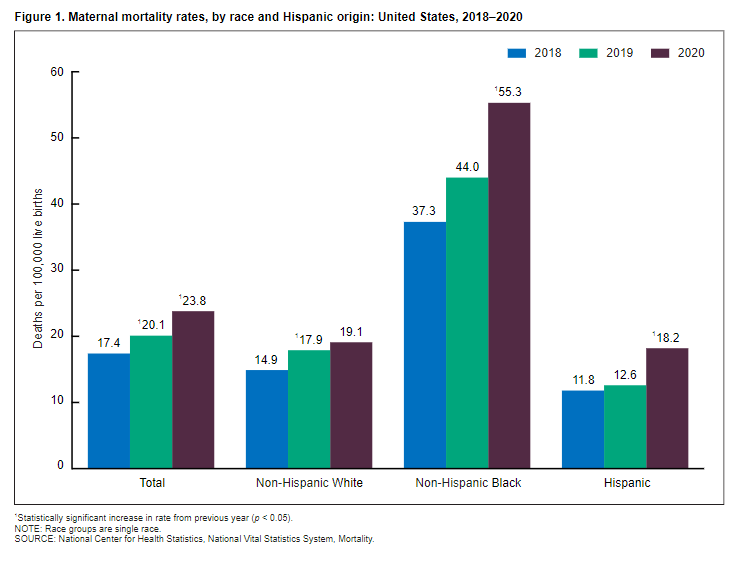
This report updates a previous one that showed maternal mortality rates for 2018 and 2019 (2). In 2020, 861 women were identified as having died of maternal causes in the United States, compared with 754 in 2019 (3). The maternal mortality rate for 2020 was 23.8 deaths per 100,000 live births compared with a rate of 20.1 in 2019 (Table). In 2020, the maternal mortality rate for non-Hispanic Black women was 55.3 deaths per 100,000 live births, 2.9 times the rate for non-Hispanic White women (19.1) (Figure 1 and Table). Rates for non-Hispanic Black women were significantly higher than rates for non-Hispanic White and Hispanic women. The increases from 2019 to 2020 for non-Hispanic Black and Hispanic women were significant. The observed increase from 2019 to 2020 for non-Hispanic White women was not significant.
The Centers for Disease Control and Prevention has created the public concern about black maternal mortality. In February, the CDC released data showing that the maternal mortality rate for black women is 2.9 times higher than the rate for white women. It’s a worrisome statistic, yet the CDC’s own data, as well as a study from the CDC Foundation, provide crucial (and generally unreported) context.
To be clear, even a single death of a pregnant woman is one too many. But the overwhelming majority of women survive motherhood: in 2020, according to the CDC, 861 women in the United States died related to pregnancy, out of a total of about 3.6 million births—a rate of 0.02 percent. Just over 350 were white, while just under 300 were black. Scientifically speaking, it’s hard to draw society-wide conclusions from such a small sample. It’s even harder when you recognize that the CDC statistics include deaths that occurred up to a year after delivery, as well as those caused by underlying and preexisting medical conditions that pregnancy may have aggravated. And the CDC admits that the systems for identifying mortality rates are prone to error.
….
The panel found that less than about a third of the preventable deaths, across all races, were attributable to individual providers. It did not cite racial bias as the reason. Yet the academic and media narrative leads to the assumption that black mothers are dying because doctors and nurses are racist. This leads to a corresponding claim that black mothers would die less often if they saw black doctors, which some call “racial concordance.” These are strange assertions, since Hispanic maternal mortality is lower than the rate for whites, which wouldn’t be true if medical professionals were racist. Yet these claims are still being used to justify discriminatory and dangerous policies across health care.
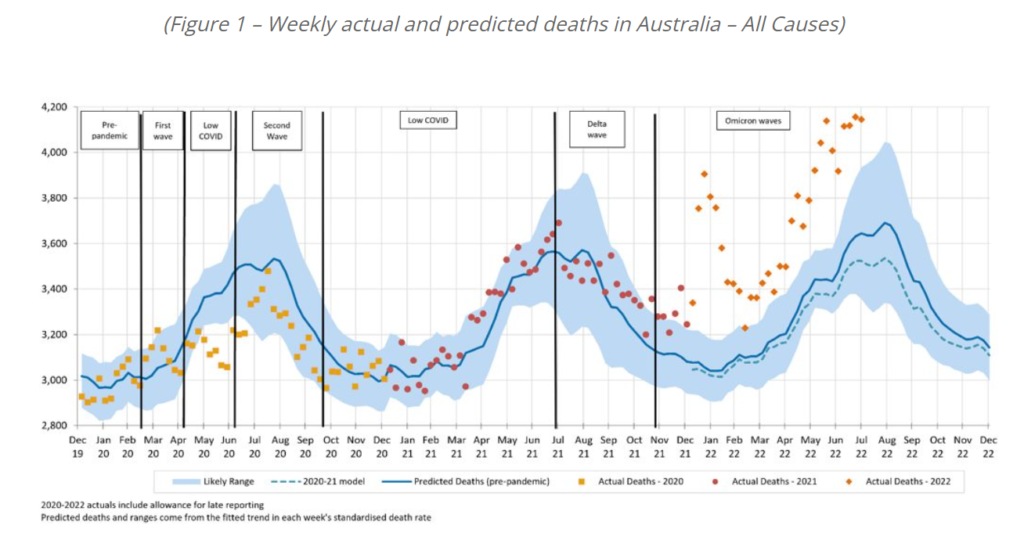
Total excess mortality for the month of July 2022 is estimated at 16% (+2,600 deaths), relative to expected mortality at pre-pandemic levels.
Total excess mortality for the first seven months of 2022 is 14% (+13,700 deaths).
Around half of the excess mortality for the first seven months of 2022 is due to COVID-19 (+7,100 deaths) with remaining excess of +6,600 due to the remaining causes.
October 2022 has the lowest COVID-19 surveillance deaths of any month in 2022.
We estimate that COVID-19 deaths will result in excess mortality of around 6% (+2,800) for August to October 2022, with overall excess mortality likely to be higher than this.
We continue to expect that COVID-19 will be the third leading cause of death in Australia in 2022.
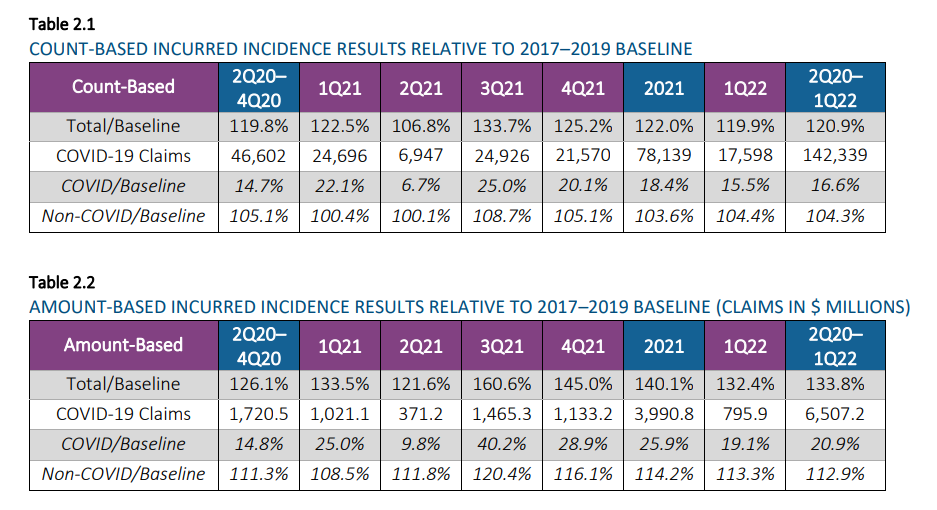
Tables 2.1 through 2.41 display high-level incidence results for the second quarter of 2020 through the first quarter of 2022 compared to the 2017-2019 baseline period for each combination of (a) incurred/reported basis and (b) count/amount basis as of March 31, 2022. In these tables, the number of COVID-19 claims has not been adjusted for seasonality, but the ratios to baseline have been adjusted for seasonality.
Note that additional data reported in April and May 2022 indicated that the 1Q 2022 excess mortality would likely complete downward from the 19.9% shown below using March data. The fully complete 1Q 2022 excess mortality is expected to remain above 15%.
….
The 24-month period of April 2020 through March 2022 showed the following Group Life mortality results: • Estimated reported Group Life claim incidence rates were up 20.0% on a seasonally-adjusted basis compared to 2017–2019 reported claims. • Estimated incurred Group Life incidence rates were 20.9% higher than baseline on a seasonally-adjusted basis. As noted above, the incurred incidence rates in February and March 2022 are based on fairly incomplete data, so they are subject to change and should not be fully relied upon at this point.
Author(s):
Thomas J. Britt, FSA, MAAA Paul Correia, FSA, MAAA Patrick Hurley, FSA, MAAA Mike Krohn, FSA, CERA, MAAA Tony LaSala, FSA, MAAA Rick Leavitt, ASA, MAAA Robert Lumia, FSA, MAAA Cynthia S. MacDonald, FSA, MAAA, SOA Patrick Nolan, FSA, MAAA, SOA Steve Rulis, FSA, MAAA Bram Spector, FSA, MAAA
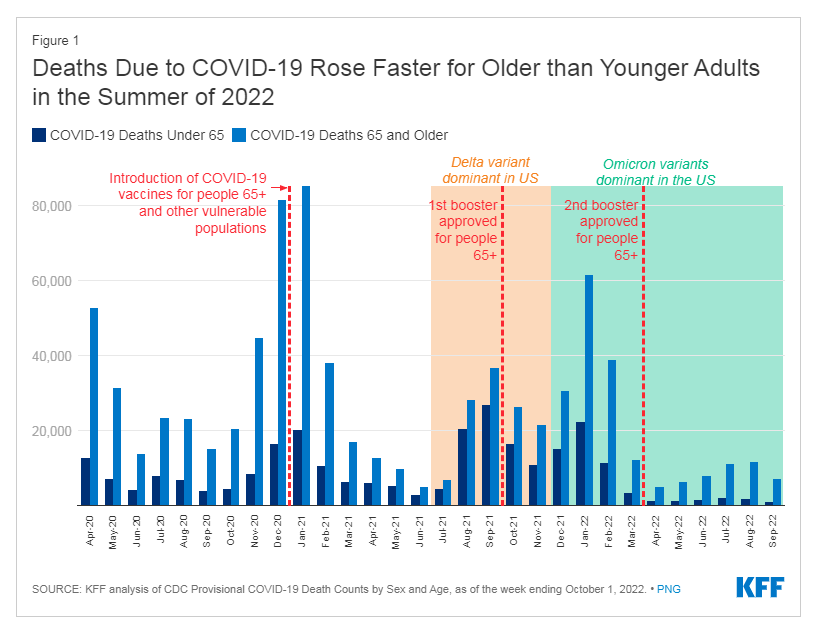
As of the week ending October 1, 2022, the United States has lost nearly 1.1 million lives to COVID-19, of which about 790,000 are people ages 65 and older. People 65 and older account for 16% of the total US population but 75% of all COVID deaths to date. Vaccinations, boosters, and treatments have led to a substantial decline in severe disease, hospitalizations, and deaths from COVID-19, but with booster uptake lagging, deaths for older adults rose again during the summer of 2022.
From April to July 2022, the number of deaths due to COVID increased for all ages but rose at a faster rate for older than younger adults and stayed high through August 2022, with deaths due to COVID topping 11,000 in both July and August among people 65 and older. While COVID deaths began to drop again in September, they were still higher for those ages 65 and older than in April or May; for those younger than 65, deaths dropped below their April levels.
The rise in deaths is primarily a function of increasing cases due to the more transmissible Omicron variant. Other factors include relatively low booster uptake, compared to primary vaccination, and waning vaccine immunity, underscoring the importance of staying up to date on vaccination. On September 1st, CDC recommended a new, updated booster for all those ages 12 and older, but particularly for those who are older.
Author(s): Meredith Freed Follow @meredith_freed on Twitter , Tricia Neuman Follow @tricia_neuman on Twitter , Jennifer Kates Follow @jenkatesdc on Twitter , and Juliette Cubanski Follow @jcubanski on Twitter
What did this new study show about the effectiveness of colonoscopies?
In this study, about 12,000 people in Sweden, Poland and Norway got colonoscopies. They saw a 31% reduction in their risk of colon cancer and a 50% reduction in their risk of dying from colon cancer compared with people who were not invited to get a colonoscopy.
Was that about what would be expected?
Some US studies have suggested that colonoscopies are even more effective. One study followed nearly 90,000 health care professionals for 22 years. Some of them chose to receive a screening colonoscopy, and some did not. The researchers estimated that screening colonoscopy was associated with a 40% reduction in the risk of getting colon cancer and a 68% reduction in the risk of dying of colon cancer.
Why would there be different success rates in the three European countries compared with the US?
Dominitz says one reason might be that most people in the European study didn’t have sedation when they got their colonoscopies. Only 23% of the patients in the European study received sedation, but virtually everyone having a colonoscopy in the US gets it. Colonoscopies can be uncomfortable, and doctors might, without even realizing it, be less thorough if people are in pain. Thoroughness – getting the scope into the folds and crevices of the colon – is important for finding growths called polyps. The more polyps doctors are able to find, the more they can reduce the person’s risk of being diagnosed with or dying from colon cancer.
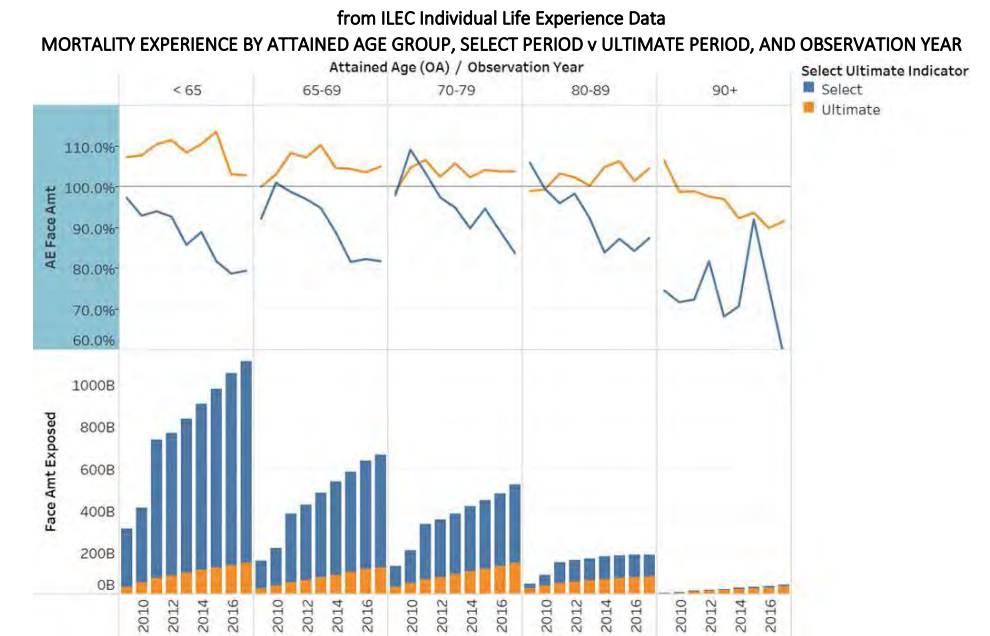
The Society of Actuaries (SOA) Research Institute released a report that examines older age mortality (OAM) with a focus on attained ages 70 and above. The report helps determine whether refinements were needed in the 2015 Valuation Basic Tables. Analysis was performed by sex, issue age and attained age, issue year cohorts, smoking risk classification, benefit band, select vs ultimate period, and interactions.
Author(s):
Old Age Mortality Subgroup of the Individual Life Experience Committee
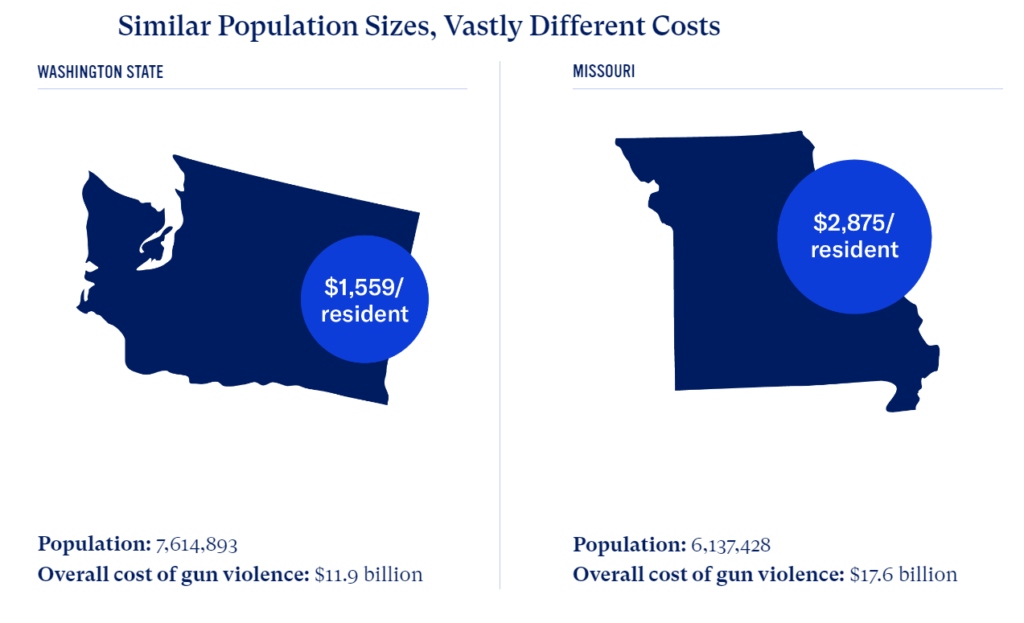
Taxpayers, survivors, families, and employers pay an average of $7.79 million daily in health care costs, including immediate and long-term medical and mental health care, plus patient transportation/ambulance costs related to gun violence, and lose an estimated $147.32 million per day related to work missed due to injury or death.
American taxpayers pay $30.16 million every day in police and criminal justice costs for investigation, prosecution, and incarceration.
Employers lose an average of $1.47 million on a daily basis in productivity, revenue, and costs required to recruit and train replacements for victims of gun violence.
Society loses $1.34 billion daily in quality-of-life costs from the suffering and lost well-being of gun violence victims and their families.
Objectives Balance quickly diminishes after the mid-50s increasing the risk for falls and other adverse health outcomes. Our aim was to assess whether the ability to complete a 10- s one-legged stance (10-second OLS) is associated with all-cause mortality and whether it adds relevant prognostic information beyond ordinary demographic, anthropometric and clinical data.
Methods Anthropometric, clinical and vital status and 10-s OLS data were assessed in 1702 individuals (68% men) aged 51–75 years between 2008 and 2020. Log-rank and Cox modelling were used to compare survival curves and risk of death according to ability (YES) or inability (NO) to complete the 10-s OLS test.
Results Overall, 20.4% of the individuals were classified as NO. During a median follow-up of 7 years, 7.2% died, with 4.6% (YES) and 17.5% (NO) on the 10-s OLS. Survival curves were worse for NO 10-s OLS (log-rank test=85.6; p<0.001). In an adjusted model incorporating age, sex, body mass index and comorbidities, the HR of all-cause mortality was higher (1.84 (95% CI: 1.23 to 2.78) (p<0.001)) for NO individuals. Adding 10-s OLS to a model containing established risk factors was associated with significantly improved mortality risk prediction as measured by differences in −2 log likelihood and integrated discrimination improvement.
Conclusions Within the limitations of uncontrolled variables such as recent history of falls and physical activity, the ability to successfully complete the 10-s OLS is independently associated with all-cause mortality and adds relevant prognostic information beyond age, sex and several other anthropometric and clinical variables. There is potential benefit to including the 10-s OLS as part of routine physical examination in middle-aged and older adults.
Author(s): Araujo CG, de Souza e Silva CG, Laukkanen JA, et al
Publication Date:
Publication history Accepted April 19, 2022 First published June 21, 2022. Online issue publication August 24, 2022
Publication Site: British Journal of Sports Medicine
Citation:
Araujo CG, de Souza e Silva CG, Laukkanen JA, et al
Successful 10-second one-legged stance performance predicts survival in middle-aged and older individuals
British Journal of Sports Medicine 2022;56:975-980.