According to data compiled by the Centers For Disease Control, approximately one in every 5,000 vaccinated Americans has tested positive for the coronavirus. That number is probably much lower in places with significantly fewer cases — like the Northeast, Chicago, Los Angeles, and San Francisco areas, where it is probably fewer than one in 10,000.
This is the first detailed data about so-called “breakthrough” infections — positive tests from people fully vaccinated. The data suggests that politicians and public health officials are wildly overreacting to the delta variant’s effect on the already vaccinated.
Wealthy, vaccine manufacturing countries like Germany, France, and the U.S. have pledged to fully vaccinate their own populations while also sharing doses with the developing world. But it’s not clear that a sufficient number of doses currently exist for them to make good on this promise. The European Union, for example, is on track to fall far short of its goal of donating 200 million doses to non-member states by the end of the year. And as of August, COVAX, the World Health Organization’s (WHO) vaccine sharing initiative, had distributed 188 million vaccines worldwide, just 19 percent of the 1.1 billion that the WHO says are needed to end the pandemic.
The more people remain unvaccinated worldwide, the likelier it is that new variants will emerge, endangering vaccinated and unvaccinated alike.
The Biden administration’s strategy for expanding worldwide vaccine access has largely relied on pushing for vaccine patent waivers through negotiations at the World Trade Organization. But those negotiations have been stymied by strong opposition from member states of the European Union, meaning that unilateral American action may be necessary to expand vaccine access on the necessary scale.
Legally, the U.S. may already have the ability to do so. The terms between Moderna and the federal government specify that the government possesses rights to the vaccine technology developed under the contract, meaning that it can unilaterally publish or share the data with anyone. Furthermore, an essential component of the Moderna vaccine was invented and patented by U.S. government researchers, meaning that the government could threaten a patent infringement suit against Moderna if the company refuses to share its vaccine know-how.
As companies allow employees to work from home and not commute into an office, the question of where they can live will likely be raised as workers potentially will seek out cheaper options as opposed to big cities.
“It’s good for employees; they’re obviously making a choice and taking advantage of lower cost of living, cheaper housing, lower taxes and shorter commutes, so they’re going to be happier,” Moody’s Analytics chief economist Mark Zandi said.
That, in turn, will make companies address several human resources issues, such as how much they should be paying workers who live in cheaper places, Zandi said.
“For example, say I worked in New York and decided now I want to work in Vero Beach, Florida,” Zandi said. “I don’t want to go back to New York, I can do my job here no problem — but if I’m living in Vero Beach, should I get New York wages or Vero Beach wages?”
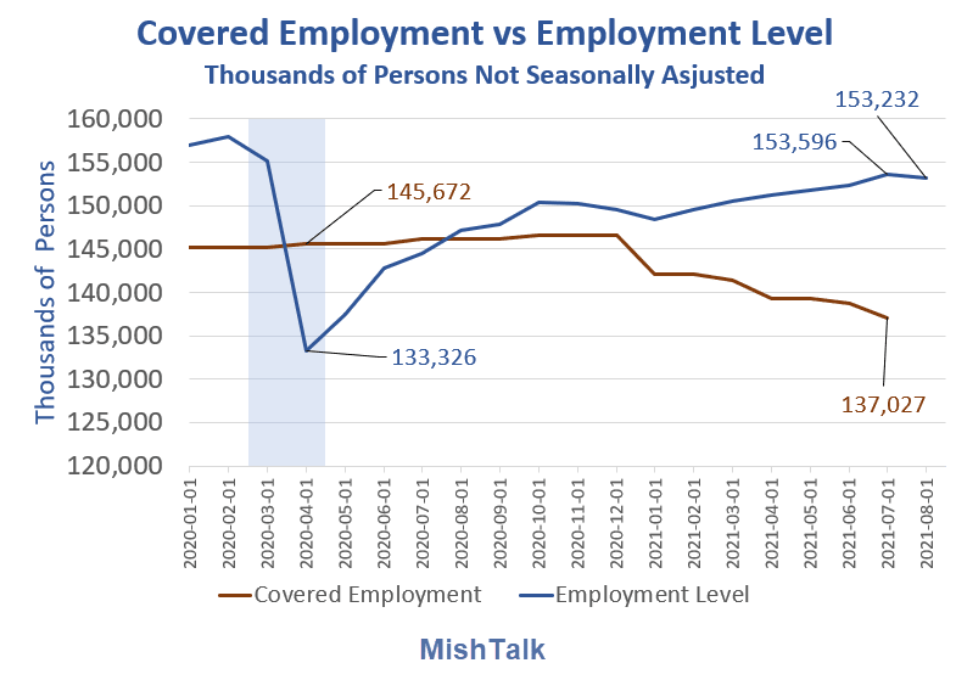
In April of 2020, there were 145.67 million people covered by unemployment insurance but only 133.33 million people working.
This unusual inversion had never happened before. It lasted 4 months, April through June of 2020.
Covered Employment data is weekly, ending Saturday and lags by a week. I use a “monthly average” which run through July vs the employment level series which runs through August.
Israel is set to begin preparations to administer fourth doses of the coronavirus vaccines as the country deals with soaring cases despite its trail-blazing roll-out of jabs.
The country’s national coronavirus czar Salman Zarka said the country needs to prepare for a fourth injection, which could be modified to better protect against new variants of the virus.
…..
‘It seems that if we learn the lessons from the fourth wave, we must consider the [possibility of subsequent] waves with the new variants, such as the new one from South America,’ he said at the time.
‘Thinking about this and the waning of the vaccines and the antibodies, it seems every few months — it could be once a year or five or six months — we’ll need another shot.’
He added that he expects Israel to be given out vaccines that had been specially adapted to cope with different variants of the virus by late 2021 or early 2022.
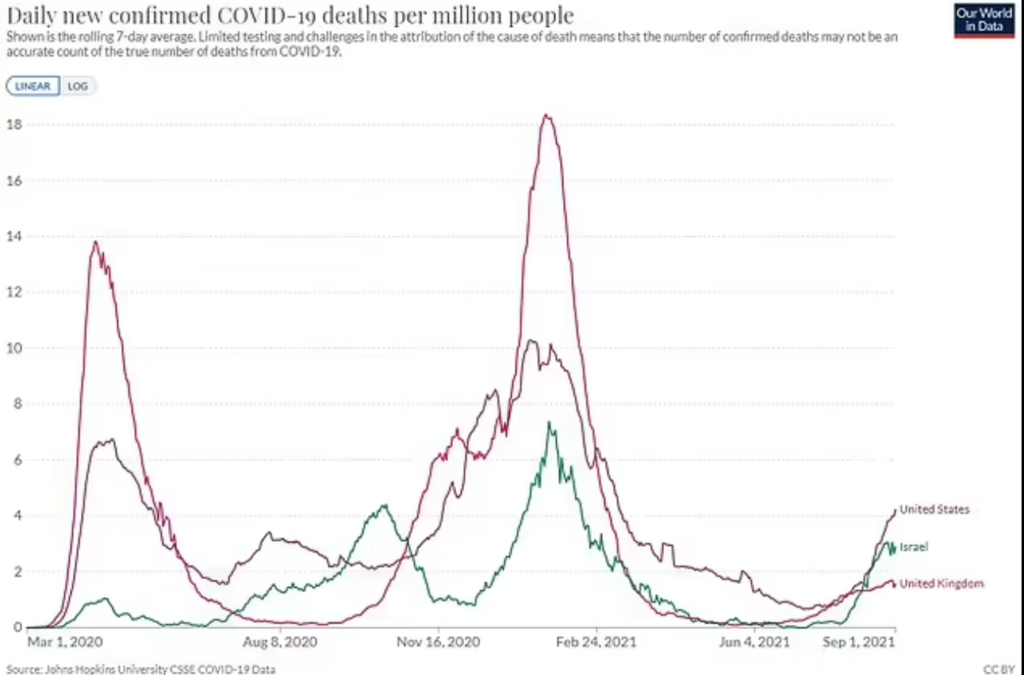
While Israel is seeing record case numbers in its fourth wave, the jabs are still protecting against severe illness with Covid deaths running at about half of the level of its second wave.
My late wife spent the last two and half years of her life in a nursing home with a form of early onset dementia. While she was in her fifties, almost everyone else there was elderly. In each of the three winters she was in the home, the place was closed to visitors at some point because of flu. This added heartbreak to heartbreak, but it was entirely reasonable. Nearly three in four flu deaths in the last pre-pandemic season occurred among seniors. Someone aged 65 or more who contracted the flu had a chance of dying of it of about one in 120. (By contrast, while more than 85% of the breakthrough deaths are among those over 65, the COVID death rate for fully vaccinated seniors is one in about 25,000.)
That is to say that the risk of death from flu in a nursing home was almost a thousand times as large as the risk of death from COVID to the overall vaccinated population, and the risk of dying from the flu if you caught it as a senior was more than 200 times greater than the risk from COVID if you are currently disease-free, similarly aged and fully vaccinated.
The Biden administration’s vaccination requirement is putting a squeeze on nursing homes as they try to balance protecting residents and retaining low-wage staff that have been reluctant to get the shot.
Later this month, the administration will outline a policy that requires all staff working at nursing homes to be vaccinated or risk the facilities losing federal funding.
The specifics of the policy are sparse so far, but it would effectively be a mandate for an industry that relies heavily on Medicare and Medicaid funding.https://aef67baff698e02f95a8ec2b0d53753d.safeframe.googlesyndication.com/safeframe/1-0-38/html/container.html
Only about 62 percent of nursing home and long term care facility staff are fully or partially vaccinated nationally, according to federal data compiled by the Centers for Medicare and Medicaid Services (CMS).
…..
“The biggest group of unvaccinated staff are certified nurse aides. They’re making close to minimum wage. They can make that, maybe even more, plus maybe even better benefits out in retail jobs, restaurant jobs. The vast majority of those employers are not imposing mandates,” Grabowski said.
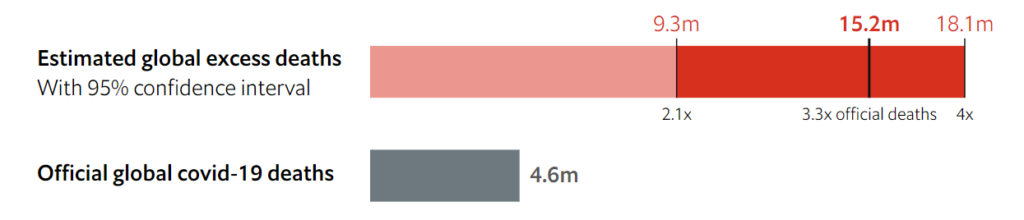
ow many people have died because of the covid-19 pandemic? The answer depends both on the data available, and on how you define “because”. Many people who die while infected with SARS-CoV-2 are never tested for it, and do not enter the official totals. Conversely, some people whose deaths have been attributed to covid-19 had other ailments that might have ended their lives on a similar timeframe anyway. And what about people who died of preventable causes during the pandemic, because hospitals full of covid-19 patients could not treat them? If such cases count, they must be offset by deaths that did not occur but would have in normal times, such as those caused by flu or air pollution.
The downloadable data sets on cases and deaths included the report date as well as the date a person died or got sick, allowing journalists and independent researchers to select the best metric for their purposes. The daily reports showed additional cases and deaths added from one day to the next.
In June, as case numbers dropped and vaccination rates continued to rise, the health department discontinued the dashboard and changed to a weekly report. The only near-daily data was submitted by the health department to the CDC and published on the CDC Trend Tracker website.
At first, the data on the CDC website was updated in a largely predictable manner, similar to the way that the DOH had reported daily changes throughout the pandemic. Then on Aug. 10, without warning or any explanation from the health department or the CDC, the data for nearly every day of the previous year changed. Neither agency immediately explained the changes.
Author(s): Sarah Blaskey, Ana Claudio Chacin and Devoun Cetoute, McClatchy Washington Bureau
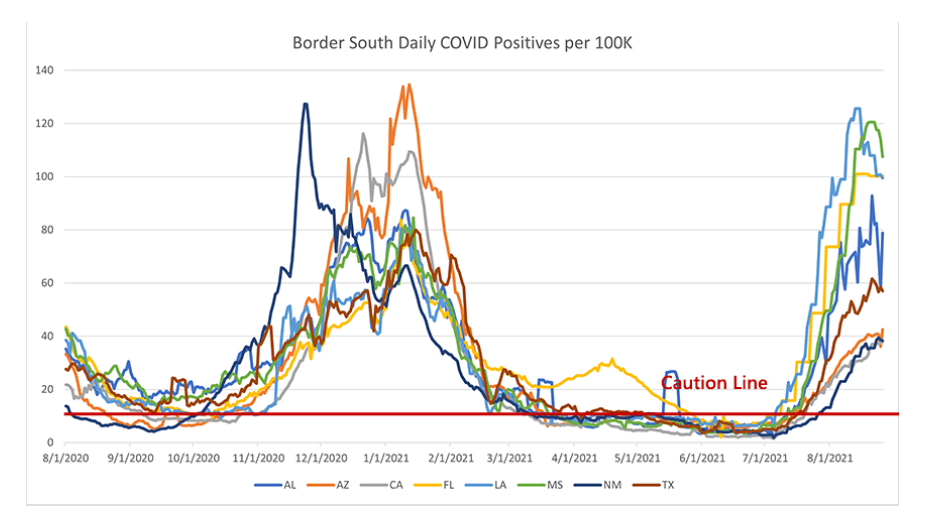
This region has been the tough one. It looks like we’re on the other side of the case surge in the worst hit states (LA, MS, FL, AL). Daily cases went up much higher than I would have expected, even higher than the winter surge. What has been truly surprising is that Florida is substantially more vaccinated than those other states, about 15-20% higher in adult vaccination and up at 95% vaccinated for seniors. That should shrink their pool of COVID-vulnerable individuals massively and reduce their death rate substantially.
And, while Florida’s death rate is lower than LA and MS, it’s not nearly at the levels we would have hoped or expected. I’m at a loss to explain this. Certain proposals have been tossed around: Florida is an older state, so more of their population is vulnerable. But their vaccination rates (nearly universal coverage among the elderly!) really should suppress this enormously. If a particular age group had +90% vaccination rates, I would expect that group’s COVID deaths to be reduced by at least 70%. Instead, the elderly are still making up the vast majority of COVID deaths in Florida.
Author(s): PoliMath, aka Matt Shapiro
Publication Date: 31 August 2021
Publication Site: Marginally Compelling at substack
Trustees for the Social Security trust fund in an annual report released Tuesday said the program is expected to pay benefits that exceed its income in 2021, the same as it anticipated last year at the outset of the pandemic.
The trustees now project elevated mortality rates related to the pandemic through 2023, and expect lower immigration and child-bearing this year and next, compared with their 2020 estimates. They also expect the pandemic has lowered worker productivity and thus economic output permanently.
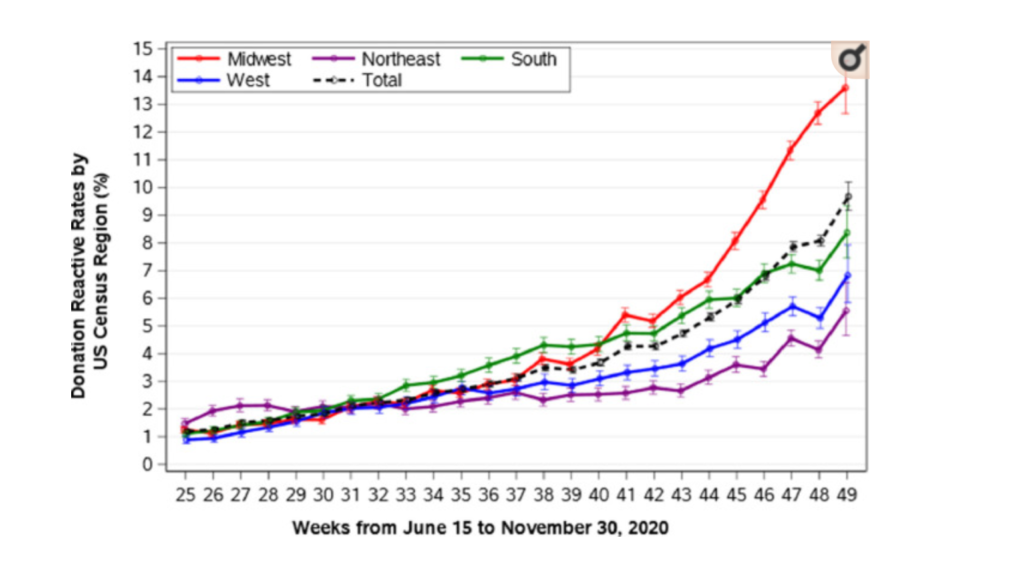
In the United States, many blood collection organizations initiated programs to test all blood donors for antibodies to SARS-CoV-2, as a measure to increase donations and to assist in the identification of potential donors of COVID-19 convalescent plasma (CCP). As a result, it was possible to investigate the characteristics of healthy blood donors who had previously been infected with SARS-CoV-2. We report the findings from all blood donations collected by the American Red Cross, representing 40% of the national blood supply covering 44 States, in order to characterize the seroepidemiology of SARS-CoV-2 infection among blood donors in the United States, prior to authorized vaccine availability. We performed an observational cohort study from June 15th to November 30th, 2020 on a population of 1.531 million blood donors tested for antibodies to the S1 spike antigen of SARS-CoV-2 by person, place, time, ABO group and dynamics of test reactivity, with additional information from a survey of a subset of those with reactive test results. The overall seroreactivity was 4.22% increasing from 1.18 to 9.67% (June 2020 – November 2020); estimated incidence was 11.6 per hundred person-years, 1.86-times higher than that based upon reported cases in the general population over the same period. In multivariable analyses, seroreactivity was highest in the Midwest (5.21%), followed by the South (4.43%), West (3.43%) and Northeast (2.90%). Seroreactivity was highest among donors aged 18-24 (Odds Ratio 3.02 [95% Confidence Interval 2.80-3.26] vs age >55), African-Americans and Hispanics (1.50 [1.24-1.80] and 2.12 [1.89-2.36], respectively, vs Caucasian). Group O frequency was 51.5% among nonreactive, but 46.1% among seroreactive donors (P< .0001). Of surveyed donors, 45% reported no COVID-19-related symptoms, but 73% among those unaware of testing. Signal levels of antibody tests were stable over 120 days or more and there was little evidence of reinfection. Evaluation of a large population of healthy, voluntary blood donors provided evidence of widespread and increasing SARS-CoV-2 seroprevalence and demonstrated that at least 45% of those previously infected were asymptomatic. Epidemiologic findings were similar to those among clinically reported cases.
Author(s): Roger Y Dodd, Bryan R Spencer, Meng Xu 1, Gregory A Foster 1, Paula Saá 1, Jaye P Brodsky 2, Susan L Stramer 3