Graphic:
Excerpt:
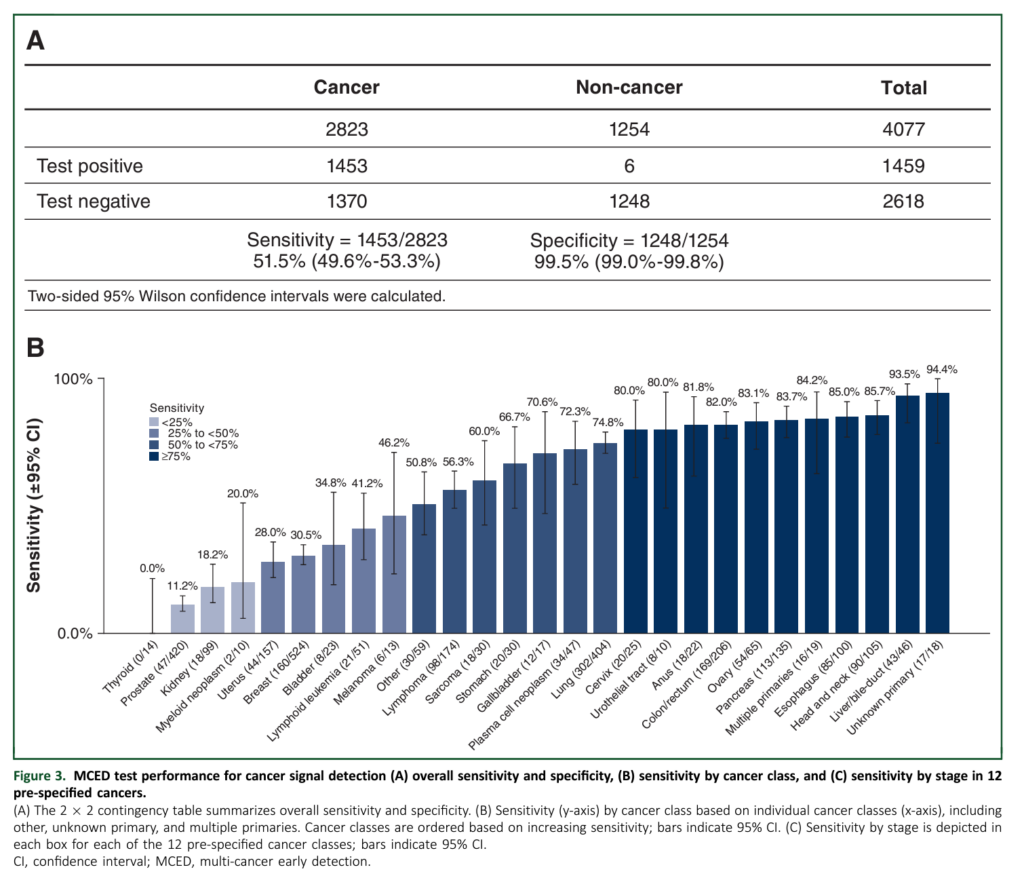
Looking a bit more closely you see why Grail’s test is actually useless, or dangerous, or both. Let’s start with the sensitivity of the test. For a cancer screening test to work, it must find disease before it has caused symptoms — when it is in an early or premalignant stage. Say what you want about lung cancer screening, mammography, PSA, and colonoscopy (I’m talking to you Drs. M and P) but at least they look for, and succeed at finding, early stage/premalignant disease. Here is the sensitivity of the Galleri test by stage: stage 1, 16.8%; stage 2, 40.4%; stage 3, 77%; stage 4, 90.1%.
The test is nearly worthless at finding stage 1 disease, the stage we would like to find with screening. The type of disease that is usually cured with surgery alone.
How about specificity? Let’s consider a fictional, 64-year-old male patient who presents to his internist worried about pancreatic cancer. I pick pancreatic not only because it is a scary cancer: we can’t screen for it, our treatments stink, and it seems to kill half the people in NYT obituary section. I also chose it because it is the anecdotal disease in the WSJ article.
….
Working through the math (prevalence 0.03%, sensitivity 61.9%, specificity 99.5%), this means our patient’s likelihood of having pancreatic cancer after a positive test is only 3.58%. For our patient, we have caused anxiety and the need for an MRI. You almost hope to find pancreatic cancer at this point to be able to say, “Well, it was all worth it.” If the MRI or ERCP is negative, the patient will live with fear and constant monitoring. (You will have to wait until next week to consider with me the impact of this test if we were to deploy it widely).
If the evaluation is positive, and you have managed to diagnose asymptomatic, pancreatic cancer, the likelihood of survival is probably, at best, 50%.
Let’s end this week with two thoughts. First the data for the Galleri test is not good, yet. The test characteristics are certainly not those we would like to see for a screening test. Even more importantly, good test characteristics are just the start. To know that a test is worthwhile, you would like to know that it does more good than harm. This has not even been tested. The WSJ article scoffs at the idea that we would want this data.5
Author(s): Adam Cifu, MD
Publication Date: 15 Feb 2024
Publication Site: Sensible Medicine, substack