In the United States, the number of cases and deaths that had been rising to a peak for almost a year have been flattening out, thanks, in large part, to COVID-19 vaccinations that began in December. As the weeks pass, more reports have been coming out about the effectiveness of the vaccines that are in use and the potential of those still in development. So, how do they differ?
It’s important to keep up, but it’s also a daunting task, given the flood of information (and misinformation) coming at us from so many directions.
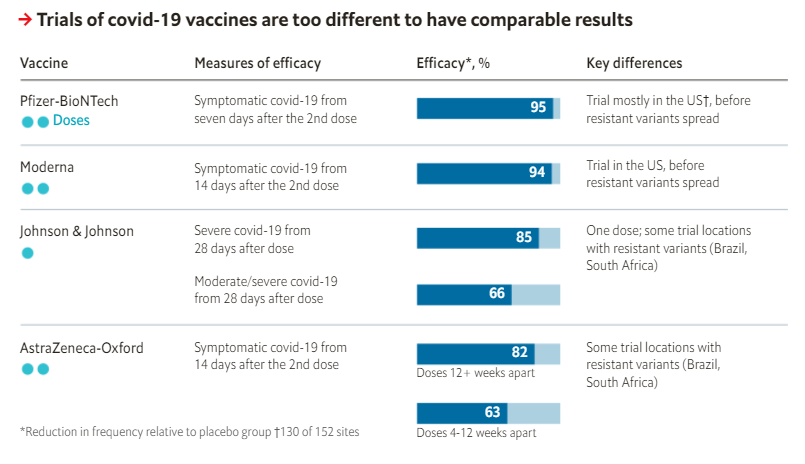
Vaccines from Pfizer-BioNTech, Moderna, and Johnson & Johnson are being administered in the U.S. right now, and others are on track to do the same.
We mapped out a comparison of the most prominent COVID-19 vaccines.
Author(s): Kathy Katella
Publication Date: 1 July 2021 (originally published February 2021, updated)
The UK has four vaccines approved for use: Pfizer-BioNTech, Oxford-AstraZeneca, Moderna and Janssen; three of which require two doses for maximum protection.
The campaign to reach as many people as quickly as possible was boosted by a shift in policy in early January – to prioritise the first dose of a vaccine, with a second dose up to 12 weeks later, a bigger gap than originally planned.
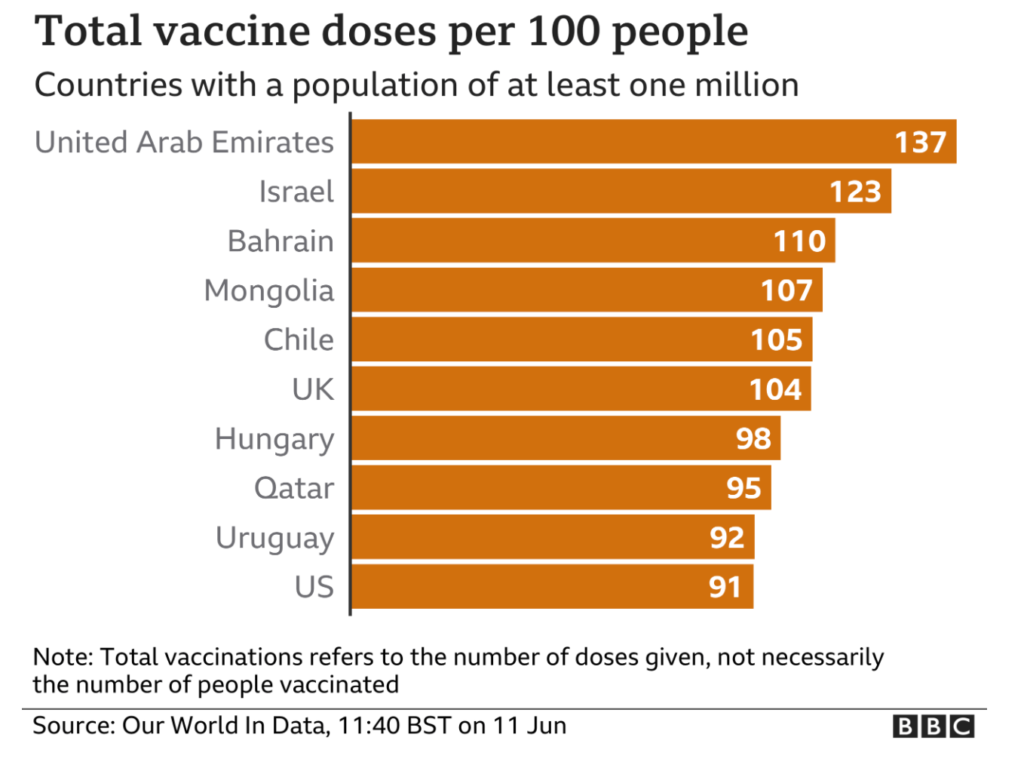
Progress made in the UK so far means the country continues to be among those with the highest vaccination rates globally.
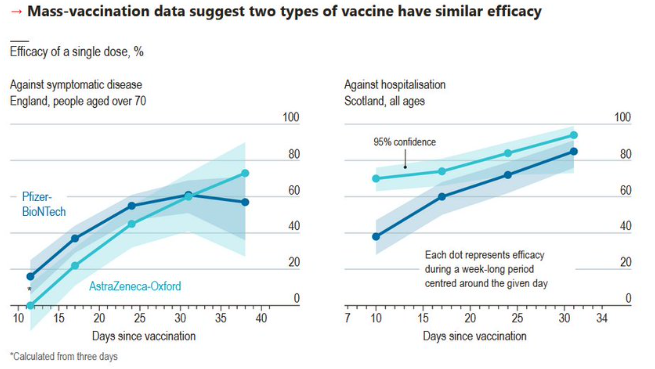
The good news? Vaccines still sharply reduce the risk of being admitted to hospital with the Delta variant. The Scottish study found that the Pfizer/BioNTech vaccine provided 79% protection, two weeks on from the second dose, while the Oxford/AstraZeneca vaccine offered 60% protection. That lower rate may be due to the fact that it takes longer for immunity to develop with the Oxford/AstraZeneca vaccine, researchers said.
However, research released shortly after by Public Health England was even more promising. It found that the Pfizer/BioNTech vaccine provides 96% protection from hospitalization after two doses, while the Oxford/AstraZeneca is 92% effective at preventing hospitalization after both shots. The conclusion? It’s yet more evidence of the importance of making sure as many people as possible get vaccinated, and that they get both shots.
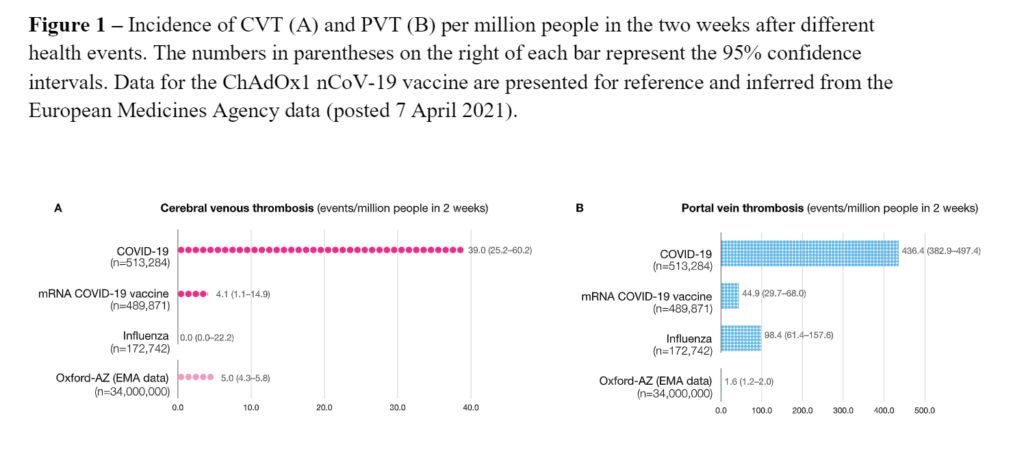
Using an electronic health records network we estimated the absolute incidence of cerebral venous thrombosis (CVT) in the two weeks following COVID-19 diagnosis(N=513,284), or influenza (N=172,742), or receipt of the BNT162b2 or mRNA-1273 COVID-19 vaccines(N=489,871). The incidence of portal vein thrombosis (PVT) was also assessed in these groups, as well as the baselineCVTincidence over a two-week period. The incidence of CVT after COVID-19 diagnosis was 39.0 per million people (95% CI, 25.2–60.2). This was higher than the CVT incidence after influenza (0.0 per million people, 95% CI 0.0–22.2, adjusted RR=6.73, P=.003) or after receiving BNT162b2 or mRNA-1273 vaccine (4.1 per million people, 95% CI 1.1–14.9, adjusted RR=6.36, P<.001). The relative risks were similar if a broader definition of CVT was used. For PVT, the incidence was 436.4 per million people (382.9-497.4) after COVID-19, 98.4 (61.4-157.6) after influenza, and 44.9 (29.7-68.0) after BNT162b2 or mRNA-1273. The incidence of CVT following COVID-19 was higher than the incidence observed across the entire health records network (0.41 per million people over any 2-week period). Laboratory test results, available in a subset of the COVID-19 patients, provide preliminary evidence suggestive of raised D-dimer, lowered fibrinogen, and an increased rate of thrombocytopenia in the CVT and PVT groups. Mortality was 20% and 18.8% respectively. These data show that the incidence of CVT is significantly increased after COVID-19, and greater than that observed with BNT162b2 and mRNA-1273 COVID-19 vaccines. The risk of CVT following COVID-19 is also higher than the latest estimate from the European Medicines Agency for the incidence associated withChAdOx1 nCoV-19 vaccine (5.0 per million people, 95% CI 4.3–5.8). Although requiring replication and corroboration, the present data highlight the risk of serious thrombotic events in COVID-19, and can help contextualize the risks and benefits of vaccination in this regard.
Author(s): Maxime Taquet, Masud Husain, John R Geddes, Sierra Luciano, Paul J Harrison
A study by Oxford University found the number of people who receive blood clots after getting vaccinated with a coronavirus vaccine are about the same for those who get Pfizer PFE, 2.43% and Moderna MRNA, 6.67% vaccines as they are for the AstraZeneca AZN, -0.16% vaccine that was produced with the university’s help. According to the study, 4 in 1 million people experience cerebral venous thrombosis after getting the Pfizer or Moderna vaccine, versus 5 in 1 million people for the AstraZeneca vaccine. The risk of getting CVT is much higher for those who get COVID-19 — 39 in a million patients — than it is for those who get vaccinated. AstraZeneca’s vaccine use has been halted or limited in many countries on blood clot concerns.
The University of Oxford said it has paused administering doses of the Covid-19 vaccine it developed with AstraZeneca PLC in a small U.K. study to test the shot in children and teenagers, pending further information about rare blood-clotting issues in adults who have received it.
The Oxford-led pediatric trial started in mid-February and is aimed at testing the vaccine in more than 200 young people aged 6 to 17 years. An Oxford spokesman said Tuesday that no safety issues have arisen in the trial itself, but broader concerns about rare clotting problems in adults have triggered further regulatory reviews in the U.K. and Europe to investigate any potential link with the vaccine.
Oxford is waiting for more information from the U.K.’s drugs watchdog, the Medicines and Healthcare products Regulatory Agency, before giving any further vaccinations to children or teenagers in the pediatric trial, the spokesman said.
The pause is the latest setback for the Oxford-AstraZeneca shot, which has faced questions about its efficacy and potential side effects even as tens of millions of doses have been administered following safety signoffs in more than 70 countries.
Supported by Angela Merkel, the German chancellor, the EU Commission (its administrative arm) took over the negotiations with vaccine manufacturers on behalf of all EU member-states last June. This was designed both as a declaration of EU “solidarity” and because of the belief that bargaining on behalf of the whole bloc could secure the vaccine at a cheaper price, a calculation that appeared to take little account of the economic costs of any delays, and delay was what — for a variety of reasons — Brussels delivered.
The U.K. came to its deal with AstraZeneca (the manufacturer of the Oxford vaccine) three months earlier than the EU, and its contract came with sharper teeth. The EU also took four months longer than the U.K. and U.S. to sign up with Pfizer.
Making matters worse, the EU’s FDA, the European Medicines Agency (EMA), a body by definition particularly receptive to the precautionary principle that plays such a dominant role in EU policy-making (except when it comes to setting up a new currency), took its time to approve the first vaccines. Its first approval came some weeks after the U.K. and ten days or so after the U.S.
Aside from finding the vaccine 79% effective, the preliminary results indicated the vaccine was even more effective in study subjects ages 65 years and older, and the shot was safe.
The late-stage, or Phase 3, trial had 32,449 subjects in the U.S., Peru and Chile. About 20% of them were 65 years or older.
The fuller data showed the vaccine to be 85% effective in the older age group. Older adults are considered more vulnerable to serious Covid-19, making them a high-priority group in vaccinations globally.
Though AstraZeneca’s latest release involved more cases, the company’s analysis might still be incomplete. AstraZeneca said it was reviewing an additional 14 cases to see if they should be added to the final tally.
Last week Austria, Norway, Denmark, and Iceland all suspended the administration of the Oxford-AstraZeneca COVID-19 vaccine, citing reports of blood clots occurring in a few folks who had been inoculated with it. Ireland, France, Germany, Italy, Spain, Thailand, and the Netherlands have now joined them.
“There is no causal effect established or anything like that yet,” Irish Prime Minister Micheal Martin told CNBC, “but as a precautionary move in line with the precautionary principle and in an abundance of caution, our clinical advice was to pause the program whilst the EMA does a review of this.”
The precautionary principle is an ideological construct that eschews risk-benefit evaluations and essentially requires that all new technologies be somehow proved entirely risk-free before they can be used.
Italy blocked the export of AstraZeneca PLC’s Covid-19 vaccine to Australia, in a move coordinated with European Union authorities, reflecting mounting frustration in Europe with slow deliveries of vaccines.
The move was prompted by the persisting shortage of vaccines in Italy and the EU, delays in the supply of vaccines by AstraZeneca and the fact that Australia is considered a “nonvulnerable country” to Covid-19 under EU regulations, Italy’s Ministry of Foreign Affairs said.
The decision affects 250,700 doses, a number the ministry said was high compared with what has been delivered so far by AstraZeneca. The doses were bottled at a factory near Rome that is part of the company’s supply chain. AstraZeneca has delivered around 1.5 million doses to Italy, according to the government.
Europe’s reluctance to distribute millions of doses of AstraZeneca PLC’s Covid-19 vaccine is coming under pressure after the French government authorized use of the shot for some older people.
The French government announced it would allow people with comorbidities between the ages of 65 and 74 to receive the vaccine developed by Oxford University and AstraZeneca. New data from the U.K. on Monday showed just one dose of the vaccine was effective in preventing disease and deaths among adults aged 70 and older who had received it.
France’s move was a sharp departure from a month ago when President Emmanuel Macron told reporters that the vaccine was quasi ineffective for people older than 65, without providing evidence to back up his claim. The comments helped sow doubts across the European Union that still persist.