During the months preceding the surge of SARS-CoV-2 infections this fall and winter, many public health officials expressed concern about the potential for a “double-barreled” respiratory virus season. In this scenario, healthcare facilities would be totally overwhelmed by: 1) patients afflicted by infections caused by endemic respiratory viruses (such as influenza) that occur during any normal year, and 2) a massive influx of coronavirus patients. Fortunately, such a catastrophe did not come to pass. The reason for this is an unprecedented reduction in flu prevalence for the 2020–21 season.
…..
So perhaps a biological process, whereby viruses engage in some form of competition, or interactions, can better explain disappearances such as those currently being observed.
Subsequent research has borne out real world examples related to the phenomenon described by Simpson. According to a group of researchers at Yale, it is likely that a 2009 autumn rhinovirus epidemic interrupted the spread of influenza. The authors of that study write: “one respiratory virus can block infection with another through stimulation of antiviral defenses in the airway mucosa”. Results from another study, conducted in mice, support those findings. Mice were infected with either a rhinovirus or a murine coronavirus, and it was found that both attenuated influenza disease. Moreover, it was observed that the murine coronavirus infection reduced early replication of the influenza virus. In another study, negative interactions between noninfluenza and influenza viruses were suggested. According to the authors: “when multiple pathogens cocirculate this can lead to competitive or cooperative forms of pathogen–pathogen interactions. It is believed that such interactions occur among cold and flu viruses”. A recently published study examining the effects of interactions between an adenovirus and influenza in mice suggested that certain respiratory infections could impede “other viruses’ activities within the respiratory tract without attacking unrelated viruses directly”. Finally, in a paper entitled “A systematic approach to virus–virus interactions”, the authors state: “increasing evidence suggests that virus–virus interactions are common and may be critical to understanding viral pathogenesis”.
Between August and mid-December of 2020, at least one-quarter of large bond issuances in the municipal market involved some form of deficit financing, according to an analysis by Municipal Market Analytics (MMA). The firm analyzed 442 municipal bond issuances that totaled at least $100 million.
MMA’s Matt Fabian and Lisa Washburn added that their tally was conservative and that as many as half of those 442 issuances may have involved deficit financing because the ultimate use of the money wasn’t always clear.
“These are not typical uses of the municipal bond market, where an overwhelming majority of financing is for long-term infrastructure projects,” they told the Pew Charitable Trusts. “But last year, with state and local governments seeking as much as possible to avoid cutting spending, raising taxes, or postponing pension payments, they shifted their emphasis to short-term and temporary solutions. As the pandemic continued and federal stimulus money dried up, they increasingly took on debt for budgetary help.”
Which microbe was responsible for the Antonine Plague remains unclear, though most specialists believe that the likeliest culprit is an ancestor of the smallpox virus. The Antonine Plague is one example of a broader lesson that becomes clear in the study of human disease: Many of the most vicious microbes of human history are not altogether very old. They emerged and evolved on human time scales, in recent millenniums and centuries — and in response to the opportunities we inadvertently presented them. A second lesson is that human health and animal health are inseparable. Our relationship with the environment reverberates back upon us, sometimes with destructive force.
The smallpox virus is less than 2,000 years old. The Antonine Plague may well represent an early stage of its evolution as a human pathogen. Like many viruses, the agent of smallpox belongs to a family many of whose representatives infect small mammals, like rodents. As human societies expand, and become more interconnected, we collide with animals and their diseases. Evolution relentlessly experiments with adaptations to new hosts, and some of these experiments unfortunately prove successful.
The Antonine Plague was such an experiment. Even without understanding the microbiology of the disease, the Romans knew that the Antonine Plague had come from without, that it was something new that had appeared with terrific fury. They believed that the pestilence had been unloosed by their own soldiers on campaign beyond Roman borders, inside what is now Iraq. More likely, the germ simply spread along the bustling trade routes that connected virtually the entire Old World. The Romans carried on a vigorous commerce with East Africa, the Near East and India and China beyond. As it happens, the first documented direct contact between Rome and China fell in the very year the Antonine Plague broke out under Marcus Aurelius. Though nothing compared with our “flat” world, the Romans lived through one of the most important phases in the long history of globalization. Then as now, exposure to disease was one of its unintended consequences.
When a vaccine became available, did your dad immediately want it?
Oh, no, of course not. He was still conspiracy minded, and even to this day. But when the vaccine starts, they’re saying it’s going to be for people over 65, and my sisters said that we’ve got to get our dad to get the vaccine. We told my dad, and that’s when he started saying, I don’t need it, they’re saying that’s going to kill you, they’re saying there’s a chip. I don’t need it. I have strong blood and a positive outlook on life and insurance.
Plus, the vaccine is a vaccine of privilege. Let’s clear about that, especially the way it’s rolling out in California. You have to do it online. For weeks, there was only English, no Spanish translation. If you’re 65 and older, and especially if you’re an immigrant, more likely than not you’re not going to be the most social media–fluent of people. So not only do you need somebody you can rely on to translate any internet stuff for you, but you also need someone who’s going to have a job that allows them to be on social media nonstop. It was the luck of the draw that my sister randomly saw a friend who told her about this Instagram post with vaccine info. So she was able to do it immediately.
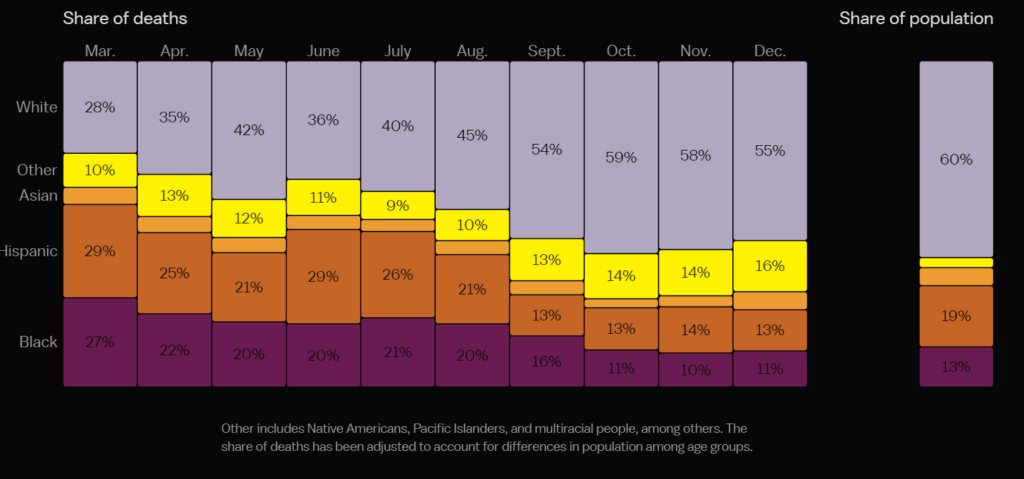
Death at this scale is difficult to comprehend, or visualize. To get a clearer sense of the shifting burden of Covid-19 deaths over time, Vox analyzed coronavirus mortality by age, region, and race from the past year, based on data from the Centers for Disease Control and Prevention and Johns Hopkins University.
We found that while Covid-19 spared no group, it impacted certain populations more than others. Throughout the pandemic, people of color have consistently been disproportionately sickened and killed by the virus. They also died young: Of Covid-19 deaths in people under the age of 45, more than 40 percent were Hispanic and about a quarter were Black.
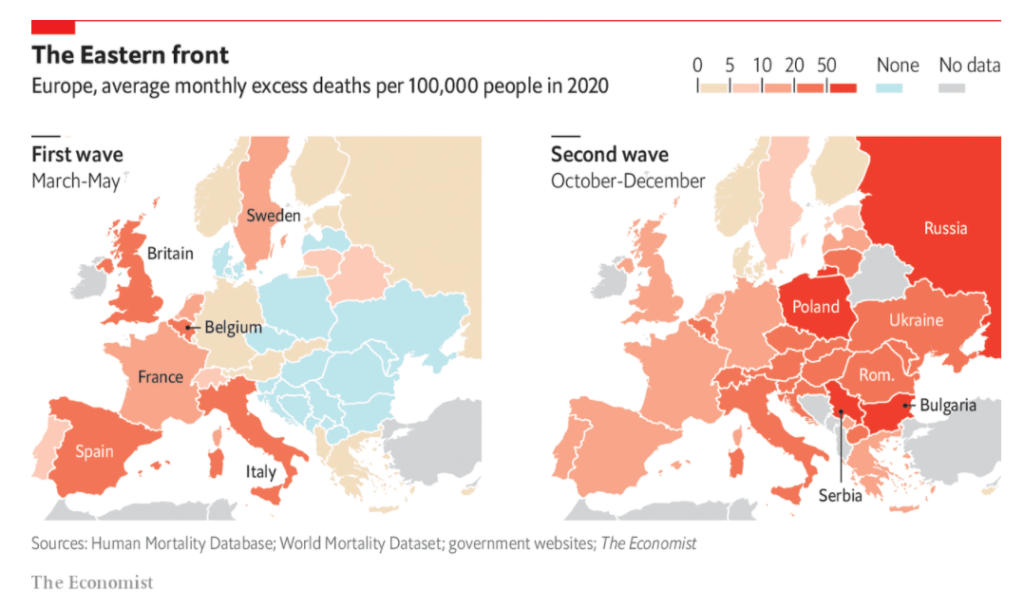
In the spring, as the virus ravaged western Europe, countries in the former eastern bloc quickly introduced border controls and lockdowns, and were largely spared. Belgium, Britain, France, Italy, the Netherlands, Spain and Sweden accounted for almost all of the continent’s deaths. Each suffered a monthly excess-mortality rate of at least 12 people per 100,000 (averaged from March to May). The country in eastern Europe that got closest was Belarus, which recorded a monthly rate of 8 per 100,000, after imposing almost no restrictions on daily life. Others were markedly lower.
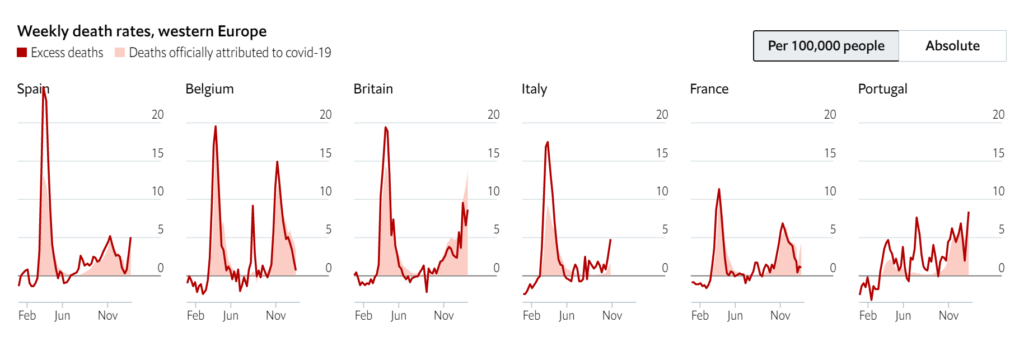
At the same time that covid-19 was devastating New York, cities in western Europe were also suffering severe outbreaks. Britain, Spain, Italy and Belgium have some of the highest national excess-death rates in the world, after adjusting for the size of their populations. France and Portugal locked down comparatively early, given the number of positive tests at the time. However, a second wave of covid-19 in winter has caused excess mortality to rise again across the region. (Some countries also recorded a small spike of non-covid fatalities during a heat wave in August.)
New York Governor Andrew Cuomo on Monday blasted state lawmakers who have threatened to rescind his emergency powers and open investigations into his administration’s coverup of its mishandling of nursing home coronavirus deaths.
“You can’t use a subpoena or the threat of investigation to leverage a person,” Cuomo said in a briefing on Monday. “That’s a crime, it’s called abuse of process, it’s called extortion.”
He also defended his earlier policy that forced nursing homes to accept coronavirus-positive patients after they were discharged from hospitals, saying that it was not sick residents who spread the virus within the nursing homes amid New York’s first wave in the spring, but visitors and staff.
Of 613 nursing homes in the state, 365 received a COVID-positive patient from the hospital, Cuomo said. Ninety-eight percent of nursing homes that admitted a patient from the hospital already had COVID in their facility before the patient was admitted, he said.
People with learning disabilities have been given do not resuscitate orders during the second wave of the pandemic, in spite of widespread condemnation of the practice last year and an urgent investigation by the care watchdog.
Mencap said it had received reports in January from people with learning disabilities that they had been told they would not be resuscitated if they were taken ill with Covid-19.
DNACPRs are usually made for people who are too frail to benefit from CPR, but Mencap said some seem to have been issued for people simply because they had a learning disability. The CQC is due to publish a report on the practice within weeks.
Federal authorities are investigating a massive counterfeit N95 mask operation in which fake 3M masks were sold in at least five states to hospitals, medical facilities and government agencies. The foreign-made knockoffs are becoming increasingly difficult to spot and could put health care workers at grave risk for the coronavirus.
These masks are giving first responders “a false sense of security,” said Steve Francis, assistant director for global trade investigations with the Homeland Security Department’s principal investigative arm. He added, “We’ve seen a lot of fraud and other illegal activity.”
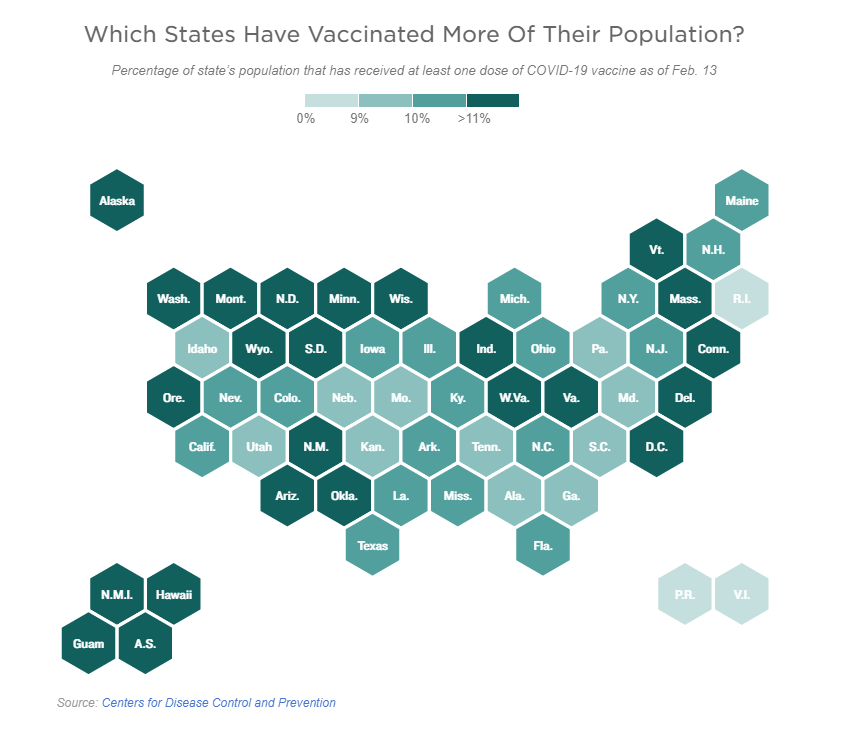
Since vaccine distribution began in the U.S. on Dec. 14, more than 50 million doses have been administered, reaching 11.2% of the total U.S. population, according to federal data collected by the Centers for Disease Control and Prevention. The U.S. is currently administering over 1.6 million shots a day.