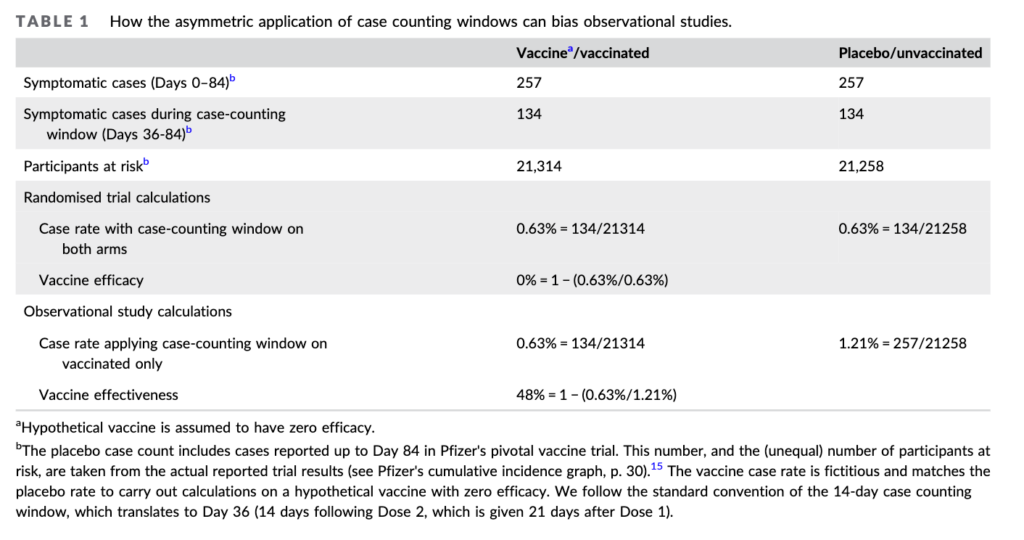
In the experiment, he says, what if we compare the control arm of the Pfizer study against an imaginary vaccine arm. And for the thought experiment assume the vaccine is useless. As the table above shows, both groups have identical numbers of covid cases— just what you would expect from a useless vaccine. A straight forward analysis shows no benefit (second to last row)
But in the ‘fictional vaccine observational study’ cases are excluded for 36 days. When this is done the useless vaccine, looks like it reduces infections by 48%!!
Doshi makes a very good point in his paper that the solution is to subtract the 36 day infection rate from the observational control arm. Sadly most investigations don’t do that.
This is one of several biases Doshi discusses, and it plagues the vaccine literature.
With the recent discovery that the CDC drafted — but never sent — a Health Alert in May 2021 about myocarditis after mRNA vaccination, I put together this timeline about vaccine myocarditis news and updates from government officials. I include a combination of documents from CDC and FDA, as well as what was covered in the mainstream media.
I think this timeline shows a pattern in which CDC & FDA failed to adequately investigate and inform the public about the risks of myocarditis early in the vaccine rollout. However, there was public acknowledgement by the CDC, as early as May 20, 2021, about a potential pattern of myocarditis after the 2nd dose of mRNA vaccines, particularly in young men.
On June 1, 2021, the CDC confirmed that they had identified a higher than expected signal of myocarditis for young men after mRNA vaccination, but that they still recommended Covid vaccination for everyone in this age group. Despite a lot more analysis and discussion of myocarditis after that, and a changing landscape with widespread natural immunity, the CDC & FDA position has changed very little since that time.
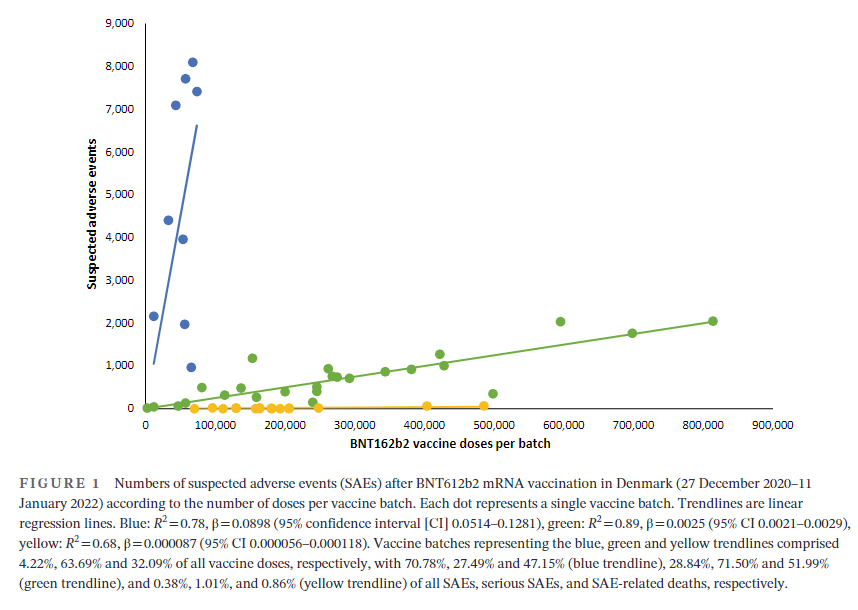
Vaccination has been widely implemented for mitigation of coronavirus disease-2019 (Covid-19), and by 11 November 2022, 701 million doses of the BNT162b2 mRNA vaccine (Pfizer-BioNTech) had been administered and linked with 971,021 reports of suspected adverse effects (SAEs) in the European Union/European Economic Area (EU/EEA).1 Vaccine vials with individual doses are supplied in batches with stringent quality control to ensure batch and dose uniformity.2 Clinical data on individual vaccine batch levels have not been reported and batch-dependent variation in the clinical efficacy and safety of authorized vaccines would appear to be highly unlikely. However, not least in view of the emergency use market authorization and rapid implementation of large-scale vaccination programs, the possibility of batch-dependent variation appears worthy of investigation. We therefore examined rates of SAEs between different BNT162b2 vaccine batches administered in Denmark (population 5.8 million) from 27 December 2020 to 11 January 2022.
….
A total of 7,835,280 doses were administered to 3,748,215 persons with the use of 52 different BNT162b2 vaccine batches (2340–814,320 doses per batch) and 43,496 SAEs were registered in 13,635 persons, equaling 3.19 ± 0.03 (mean ± SEM) SAEs per person. In each person, individual SAEs were associated with vaccine doses from 1.531 ± 0.004 batches resulting in a total of 66,587 SAEs distributed between the 52 batches. Batch labels were incompletely registered or missing for 7.11% of SAEs, leaving 61,847 batch-identifiable SAEs for further analysis of which 14,509 (23.5%) were classified as severe SAEs and 579 (0.9%) were SAE-related deaths. Unexpectedly, rates of SAEs per 1000 doses varied considerably between vaccine batches with 2.32 (0.09–3.59) (median [interquartile range]) SAEs per 1000 doses, and significant heterogeneity (p < .0001) was observed in the relationship between numbers of SAEs per 1000 doses and numbers of doses in the individual batches. Three predominant trendlines were discerned, with noticeable lower SAE rates in larger vaccine batches and additional batch-dependent heterogeneity in the distribution of SAE seriousness between the batches representing the three trendlines (Figure 1). Compared to the rates of all SAEs, serious SAEs and SAE-related deaths per 1.000 doses were much less frequent and numbers of these SAEs per 1000 doses displayed considerably greater variability between batches, with lesser separation between the three trendlines (not shown).
Author(s): Max Schmeling, Vibeke Manniche, Peter Riis Hansen
Publication Date: 30 Mar 2023
Publication Site: European Journal of Clinical Investigation
The Omicron variant of the coronavirus can partially evade the protection from two doses of Pfizer Inc (PFE.N) and partner BioNTech’s COVID-19 vaccine, the research head of a laboratory at the Africa Health Research Institute in South Africa said on Tuesday.
Still, the study showed that blood from people who had received two doses of the vaccine and had a prior infection were mostly able to neutralize the variant, suggesting that booster doses of the vaccine could help to fend off infection.
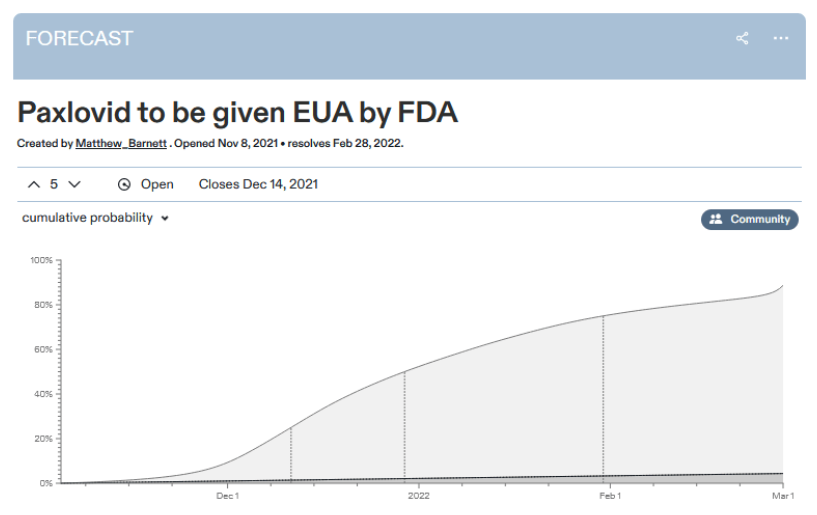
For context: a recent study by Pfizer, the pharma company backing the drug, found Paxlovid decreased hospitalizations and deaths from COVID by a factor of ten, with no detectable side effects. It was so good that Pfizer, “in consultation with” the FDA, stopped the trial early because it would be unethical to continue denying Paxlovid to the control group. And on November 16, Pfizer officially submitted an approval request to the FDA, which the FDA is still considering.
As many people including Zvi, Alex, and Kelsey have noted, it’s pretty weird that the FDA agrees Paxlovid is so great that it’s unethical to study it further because it would be unconscionable to design a study with a no-Paxlovid control group – but also, the FDA has not approved Paxlovid, it remains illegal, and nobody is allowed to use it.
One would hope this is because the FDA plans to approve Paxlovid immediately. But the prediction market expects it to take six weeks – during which time we expect about 50,000 more Americans to die of COVID.
Perhaps there’s not enough evidence for the FDA to be sure Paxlovid works yet? But then why did they agree to stop the trial that was gathering the evidence? Or perhaps there’s enough evidence, but it takes a long time to process it? But then how come the prediction markets are already 90% sure what decision they’ll make?
Pfizer Inc. and partner BioNTech SE said their Covid-19 vaccine was found to be safe in children ages 5 to 11 years in a late-stage study and generated a strong immune response in them, bringing the prospect of broader vaccination coverage closer.
Pfizer said it would share the results with regulators in the U.S. and other countries and seek emergency-use authorization in the U.S. as early as the end of the month.
The companies said the two-dose shot was found to be safe and well tolerated among the children in the study. The vaccine generated levels of antibodies that were similar to those of younger adults, meeting the study’s measurements of success, according to the companies.
Pfizer and BioNTech said they hadn’t yet determined vaccine efficacy — how well it protects against Covid-19 — for children in the age group. Not enough young subjects in the study have become sick to compare rates between children who got a vaccine and those who got a placebo, but researchers could still learn more as the trial continues.
In the United States, the number of cases and deaths that had been rising to a peak for almost a year have been flattening out, thanks, in large part, to COVID-19 vaccinations that began in December. As the weeks pass, more reports have been coming out about the effectiveness of the vaccines that are in use and the potential of those still in development. So, how do they differ?
It’s important to keep up, but it’s also a daunting task, given the flood of information (and misinformation) coming at us from so many directions.
Vaccines from Pfizer-BioNTech, Moderna, and Johnson & Johnson are being administered in the U.S. right now, and others are on track to do the same.
We mapped out a comparison of the most prominent COVID-19 vaccines.
Author(s): Kathy Katella
Publication Date: 1 July 2021 (originally published February 2021, updated)
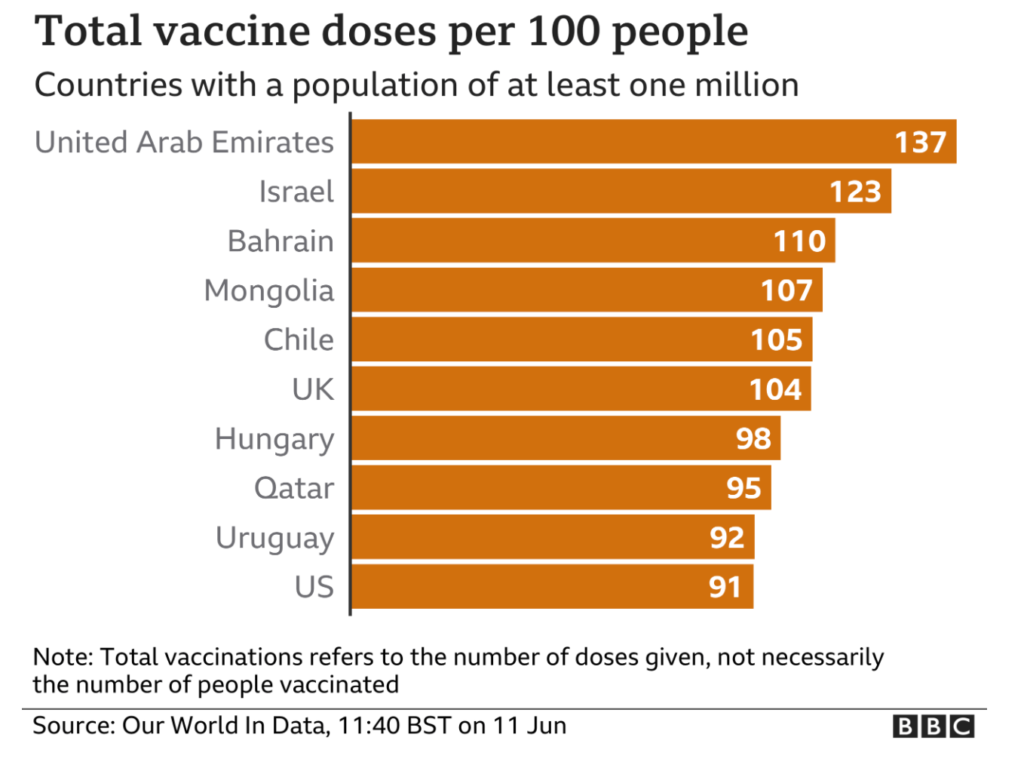
The UK has four vaccines approved for use: Pfizer-BioNTech, Oxford-AstraZeneca, Moderna and Janssen; three of which require two doses for maximum protection.
The campaign to reach as many people as quickly as possible was boosted by a shift in policy in early January – to prioritise the first dose of a vaccine, with a second dose up to 12 weeks later, a bigger gap than originally planned.
Progress made in the UK so far means the country continues to be among those with the highest vaccination rates globally.
The good news? Vaccines still sharply reduce the risk of being admitted to hospital with the Delta variant. The Scottish study found that the Pfizer/BioNTech vaccine provided 79% protection, two weeks on from the second dose, while the Oxford/AstraZeneca vaccine offered 60% protection. That lower rate may be due to the fact that it takes longer for immunity to develop with the Oxford/AstraZeneca vaccine, researchers said.
However, research released shortly after by Public Health England was even more promising. It found that the Pfizer/BioNTech vaccine provides 96% protection from hospitalization after two doses, while the Oxford/AstraZeneca is 92% effective at preventing hospitalization after both shots. The conclusion? It’s yet more evidence of the importance of making sure as many people as possible get vaccinated, and that they get both shots.
In courtrooms, mixing up the probability of “A given B’” with “B given A” is known as the “prosecutor’s fallacy”. In 1999, a court convicted Sally Clark of the murder of her two sons, in part because a medical expert claimed the chance of two accidental cot deaths was one in 73m. Even if this number was right – which it isn’t – it did not reflect the chance she was innocent. A double murder was also very rare: the relative likelihood of the two explanations was key and with new evidence and better statistical reasoning, an appeal court quashed the conviction.
There was controversy after a recent Observer headline referred to Bayes’s theorem as “obscure”. His ideas may be little known by the public, but they are growing among scientists. Many complex analyses done during the pandemic have been “Bayesian”, including modelling lockdown effects, the ONS infection survey, and Pfizer-BioNTech’s vaccine trial. The term “credible interval”, rather than “confidence interval”, is the giveaway.
Last week, Cass Business School announced the renaming of its institution after Bayes and his theorem. The obscure tomb in nearby Bunhill Fields is worth a visit.
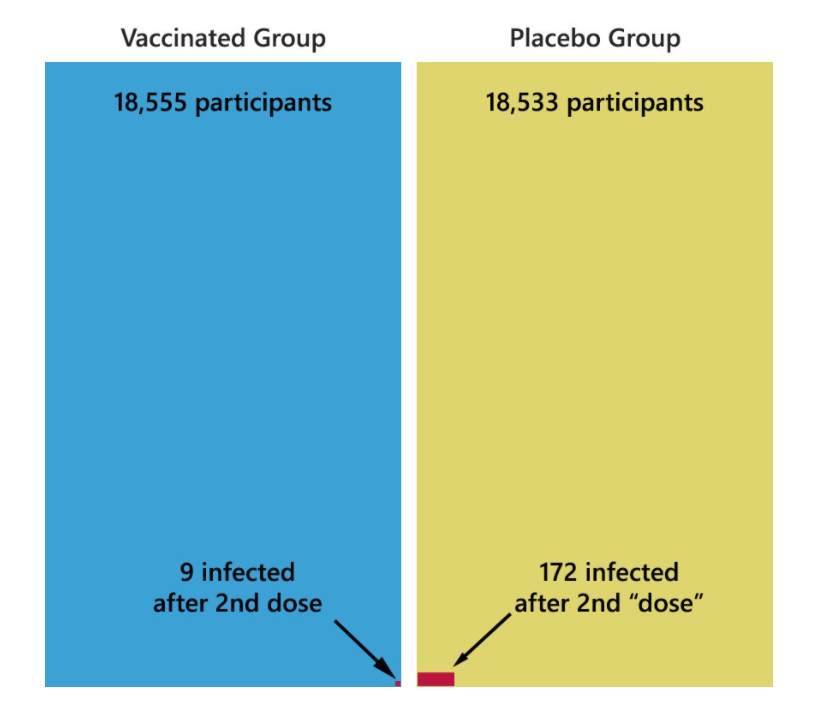
Let’s refer back to the Pfizer study submitted to the FDA. In that study, 18,555 people were vaccinated and 18,533 people received the placebo injection. In these groups, 7 days after the second dose was administered, we saw that the vaccinated group got infected at only 5% the rate that the placebo group was infected.
Furthermore, this is the number of cases we see over the course of a two month study. So those 9 people out of 18,555 were not symptomatic and infectious that whole time, but only for a few weeks.
So, to take CNN’s example and re-imagine it for the reality we have with this data.
Let’s say 1 million people are travelling. If everyone is unvaccinated (and the window of infection is roughly one week), there will be about 1,100 infected travelers.
If, however, everyone is vaccinated, there will be about 60 infected travelers and their chance of infecting you (my dear vaccinated friend) is reduced substantially.
Author(s): PoliMath
Publication Date: 13 April 2021
Publication Site: Marginally Compelling on substack