The good news? Vaccines still sharply reduce the risk of being admitted to hospital with the Delta variant. The Scottish study found that the Pfizer/BioNTech vaccine provided 79% protection, two weeks on from the second dose, while the Oxford/AstraZeneca vaccine offered 60% protection. That lower rate may be due to the fact that it takes longer for immunity to develop with the Oxford/AstraZeneca vaccine, researchers said.
However, research released shortly after by Public Health England was even more promising. It found that the Pfizer/BioNTech vaccine provides 96% protection from hospitalization after two doses, while the Oxford/AstraZeneca is 92% effective at preventing hospitalization after both shots. The conclusion? It’s yet more evidence of the importance of making sure as many people as possible get vaccinated, and that they get both shots.
The Illinois program gives people recovering from covid-19 a take-home kit that includes a pulse oximeter, a disposable Bluetooth-enabled sensor patch, and a paired smartphone. The software takes data from the wearable patch and uses machine learning to develop a profile of each person’s vital signs. The monitoring system alerts clinicians remotely when a patient’s vitals— such as heart rate—shift away from their usual levels.
Typically, patients recovering from covid might get sent home with a pulse oximeter. PhysIQ’s developers say their system is much more sensitive because it uses AI to understand each patient’s body, and its creators claim it is much more likely to anticipate important changes.
“It’s an enormous benefit,” says Terry Vanden Hoek, the chief medical officer and head of emergency medicine at University of Illinois Health, which is hosting the pilot. Working with covid cases is hard, he says: “When you work in the emergency department it’s sad to see patients who waited too long to come in for help. They would require intensive care on a ventilator. You couldn’t help but ask, ‘If we could have warned them four days before, could we have prevented all this?’”
The contribution of natural immunity should speed up the timeline for returning fully to normal. With more than 8 in 10 adults protected from either contracting or transmitting the virus, it can’t readily propagate by jumping around in the population. In public health, we call that herd immunity, defined broadly on the Johns Hopkins Covid information webpage as “when most of a population is immune.” It’s not eradication, but it’s powerful.
Without accounting for natural immunity, we are far from Anthony Fauci’s stated target of 70% to 85% of the population becoming immune through full vaccination. But the effect of natural immunity is all around us. The plummeting case numbers in late April and May weren’t the result of vaccination alone, and they came amid a loosening of both restrictions and behavior.
…..
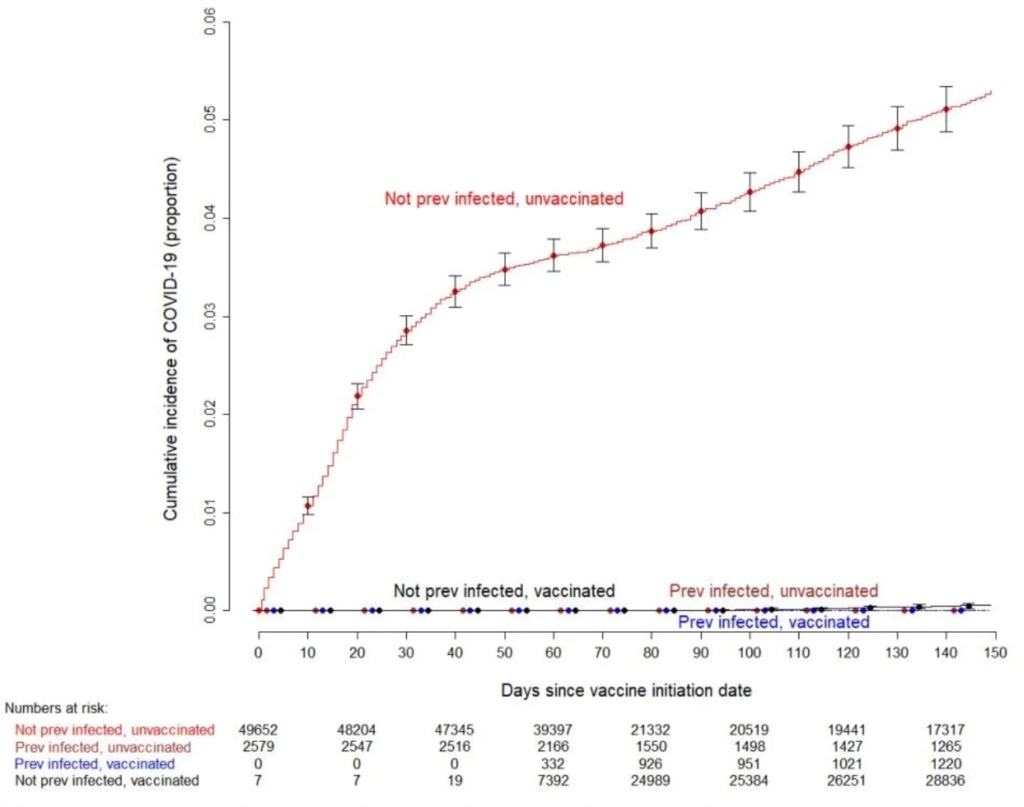
Researchers from the Cleveland Clinic published a study this week of 1,359 people previously infected with Covid who were unvaccinated. None of the subjects subsequently became infected, leading the researchers to conclude that “individuals who have had SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination.”
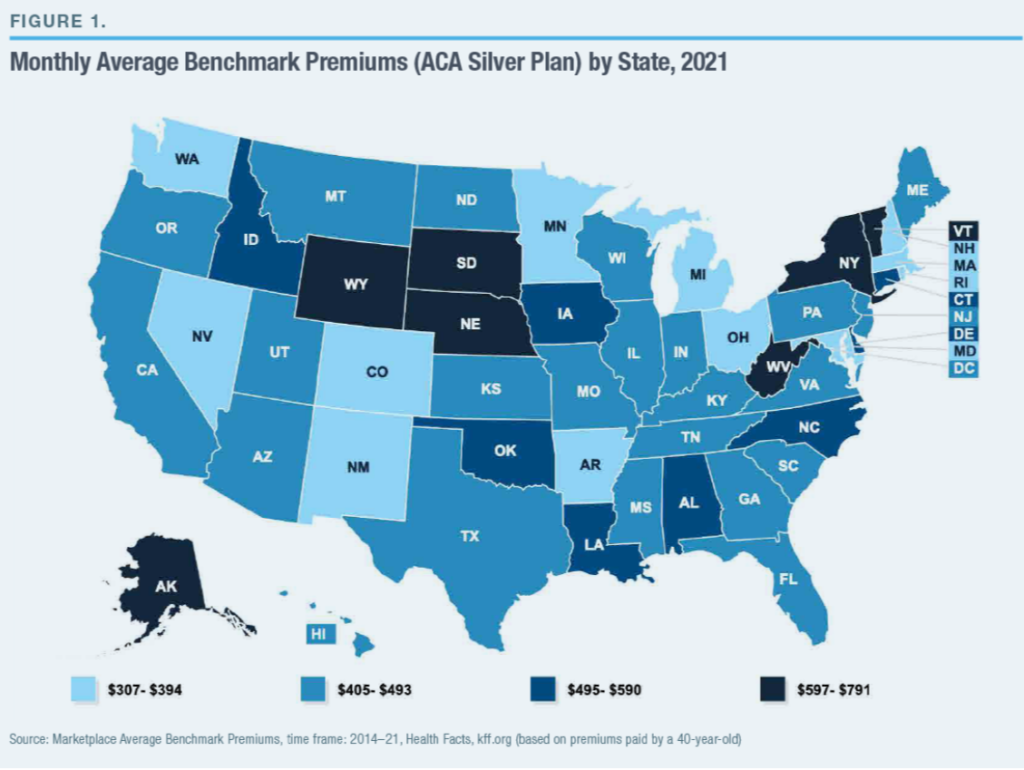
State governments often operate with limited administrative and technical resources and are highly vulnerable to lobbying by interest groups. Medical providers—physicians and hospitals—are well represented in state capitols, and they frequently push legislatures to mandate that insurers pay for services that they provide, as a way to increase the sales (and prices) of these services.
The typical state had fewer than one benefit mandate in 1970; by 2017, the average was 37. James Bailey of Temple University has estimated that each benefit mandate enacted by states tends to increase health-insurance premiums by 0.4%–1.1% and that new mandates were responsible for 9%–23% of premium increases during 1996–2011. Benefit mandates may have added value to insurance coverage by preventing insurers from leaving gaps in coverage, in order to deter sicker individuals from enrolling.[9] Still, in a study of the period 1989–94, Frank Sloan and Christopher Conover of Duke University estimated that 20%–25% of Americans without health insurance were deterred from purchasing coverage because of the added costs resulting from benefit mandates.[10]
Lobbyists for hospitals and physicians have similarly pushed states to enact laws that increase their pricing power, by making it hard for insurers to exclude them from networks of covered providers. When HMOs began to squeeze hospital costs in the late 1990s, more than 1,000 bills were introduced in state legislatures. Most states enacted laws requiring insurers to reimburse “any willing provider” for treatment according to their standard payment arrangements. A study by Maxim Pinkovskiy of the Federal Reserve Bank of New York found that anti-HMO state laws drove up the incomes of medical providers, increased service use, slowed reduction in hospital lengths of stay, and caused U.S. health-care spending to increase by 2% of GDP—accounting for much of the growth in health-insurance costs in the early 2000s.[11]
Scientists from the Cleveland Clinic, USA, have recently evaluated the effectiveness of coronavirus disease 2019 COVID-19) vaccination among individuals with or without a history of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
The study findings reveal that individuals with previous SARS-CoV-2 infection do not get additional benefits from vaccination, indicating that COVID-19 vaccines should be prioritized to individuals without prior infection. The study is currently available on the medRxiv* preprint server.
More than 300 million COVID-19 vaccines doses have now been administered in the U.S., the Centers for Disease Control and Prevention confirmed Sunday.
Why it matters: The latest CDC figures show that 41.9% of the U.S. population has been fully vaccinated against the coronavirus and 51.5% has received at least one dose.
The vaccination milestone comes as the U.S. has seen new infections fall to the lowest level since March 2020, when the pandemic began.
One success story took place in Philadelphia, thanks to an effective collaboration between two health systems and Black community leaders. Recognizing that the largely online signup process was hard for older people or those without internet access, Penn Medicine and Mercy Catholic Medical Center created a text-message-based signup system as well as a 24/7 interactive voice recording option that could be used from a land line, with doctors answering patients’ questions before appointments. Working with community leaders, the program held its first clinic at a church and vaccinated 550 people.
….
In Alabama, for example, National Guard mobile vaccination units were set up with the ultra-cold freezers needed to transport and store mRNA-based covid-19 vaccines. “Why not, when this particular push is over, leave those freezer units with the federally qualified health centers that are already in those communities?” McClure says. “You’re starting to build the infrastructure for being able to deliver vaccination on a consistent basis.”
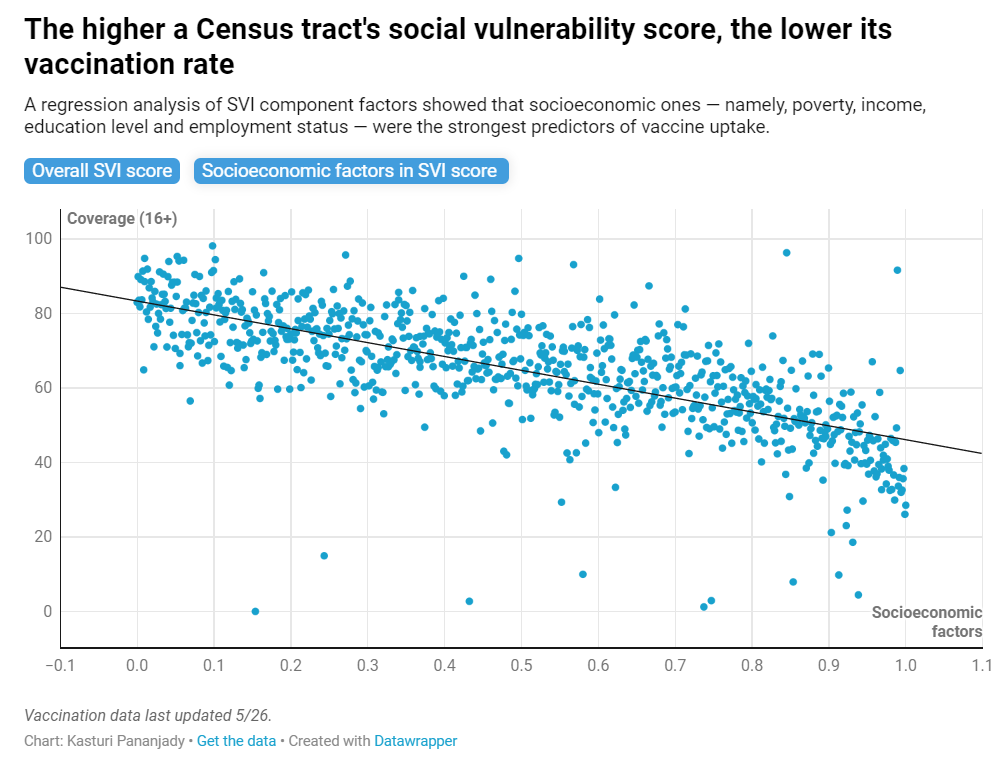
The Centers for Disease Control and Prevention’s “social vulnerability index” has formed the basis for the state’s prioritization system and has been a reliable indicator of low vaccine uptake. Generally speaking, the higher a community’s SVI score, the lower its vaccination rate, a CT Mirror analysis found.
An estimated 32% of the state’s eligible population lives in the state’s priority ZIP codes, and the state aims to administer the same percentage of vaccines within those communities. While the state inches closer to that goal each week, the statewide slowdown in the number of shots administered means that it has a lot of ground to make up. Of all the vaccines administered so far, just 25% of all vaccines distributed as of last week have gone to residents of those ZIP codes.
“Progress is slower now,” said Josh Geballe, the state’s chief operating officer, at a recent press conference.
When it comes down to it, I’ll suggest to readers that they don’t really believe that it matters. And with the Biden administration’s 2022 budget proposal comes a fairly strong indication that this is their point of view as well, that they expect, when the Trust Fund well comes dry, to simply tap general federal revenues for the necessary funds, in exactly the same manner as is done for Parts B (doctors) and D (drugs).
…..
This single sentence makes it clear that’s not the case: the only premiums paid by Medicare recipients are partial-cost payments for Parts B and D. For Part B, this is 25% of the cost for most retirees; for those with income above $85,000/$170,000 single/married, premiums are higher, reaching as much as 85% of the total cost for the highest earners. For Part D, the premium is set to cover 25.5% of the standard drug benefit, plus any extra costs charged by particular private providers for enhanced benefit levels, and an extra flat charge for higher earners. The remaining cost, 75% of Part B and 74.5% of Part D, is funded by the federal government through its general revenues.
This week’s (May 10 to May 17, 2021) pace of vaccination remained similar to last week across racial/ethnic groups. Across reporting states, vaccination rates increased by 1.3 percentage points for White people, from 40.3% to 41.6%, and by 1.2 percentage points for Black people, from 26.6% to 27.8%, maintaining the gap in rates between these groups (Figure 4). The rate for Hispanic people increased by 1.6 percentage points from 28.8% to 30.4%, while the rate for Asian people increased by 1.9 percentage points, from 50.2% to 52.1%.
Author(s): Nambi Ndugga, Olivia Pham , Latoya Hill, Samantha Artiga, Raisa Alam , Noah Parker
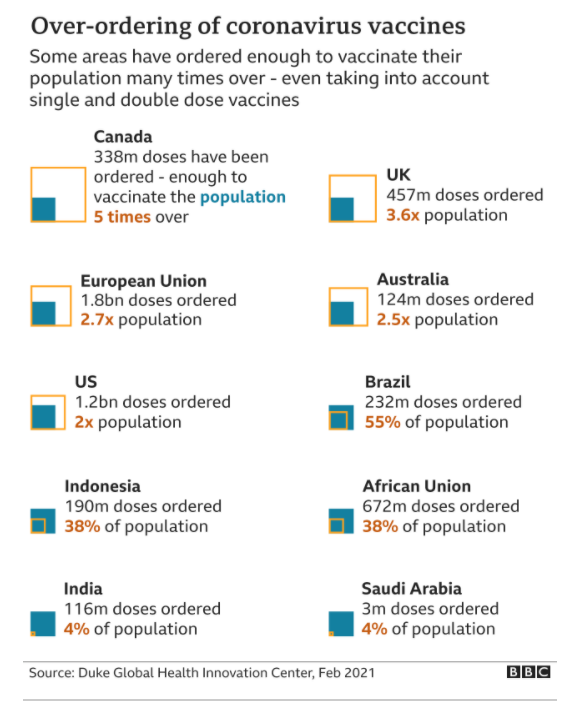
Unicef is calling on the G7 countries – Canada, France, Germany, Italy, Japan, the UK and the US, as well as the EU, to donate their surplus supplies urgently.
Some countries have ordered enough to vaccinate their population many times over, including the UK, US and Canada.
In February British Prime Minister Boris Johnson promised to donate most of the UK’s surplus supply to poorer countries but he has so far given no specific timescale. It is a similar story for the US. So far France is the only G7 country to donate doses in view of the crisis in India.