Link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10423939/
Published online 2023 Jul 31. doi: 10.3389/fneur.2023.1239182
Graphic:
Abstract:
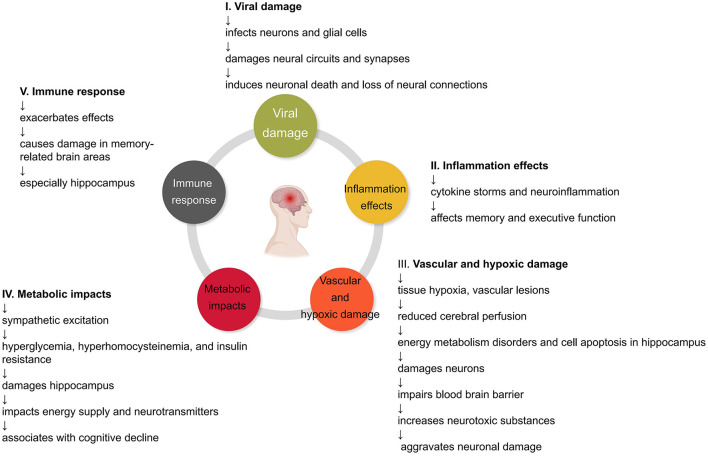
COVID-19, caused by the SARS-CoV-2 virus, is a respiratory infectious disease. While most patients recover after treatment, there is growing evidence that COVID-19 may result in cognitive impairment. Recent studies reveal that some individuals experience cognitive deficits, such as diminished memory and attention, as well as sleep disturbances, suggesting that COVID-19 could have long-term effects on cognitive function. Research indicates that COVID-19 may contribute to cognitive decline by damaging crucial brain regions, including the hippocampus and anterior cingulate cortex. Additionally, studies have identified active neuroinflammation, mitochondrial dysfunction, and microglial activation in COVID-19 patients, implying that these factors may be potential mechanisms leading to cognitive impairment. Given these findings, the possibility of cognitive impairment following COVID-19 treatment warrants careful consideration. Large-scale follow-up studies are needed to investigate the impact of COVID-19 on cognitive function and offer evidence to support clinical treatment and rehabilitation practices. In-depth neuropathological and biological studies can elucidate precise mechanisms and provide a theoretical basis for prevention, treatment, and intervention research. Considering the risks of the long-term effects of COVID-19 and the possibility of reinfection, it is imperative to integrate basic and clinical research data to optimize the preservation of patients’ cognitive function and quality of life. This integration will also offer valuable insights for responding to similar public health events in the future. This perspective article synthesizes clinical and basic evidence of cognitive impairment following COVID-19, discussing potential mechanisms and outlining future research directions.
Author(s):Zhitao Li,# 1 , 2 , † Zhen Zhang,# 3 , † Zhuoya Zhang,# 4 , † Zhiyong Wang, 3 , * and Hao Li
Publication Date: 2023 Jul 31
Publication Site: Frontiers in Neurology